INTRODUCTION
Bangladesh is a country which achieved several of the targets of health-related Millennium Development Goals (MDGs). However, there are still some challenges to reduce maternal and neonatal deaths. From 1989 to 2007, maternal mortality ratio (MMR) declined from 650 to 322 per 100,000 live births, under-five child mortality rate dropped from 133 to 65 per 1000 live births and neonatal mortality rate declined from 52 to 37 per 1000 live births (Mitra et al. 1994; NIPORT, ORC Macro, Johns Hopkins University, and ICDDR,B 2003; NIPORT, Mitra and Associates, and Macro International 2008). Despite the decreasing trend in mortality indicators, there remain inequalities in terms of socio-economic status, access in health services, access to economic development and geographic location. However, Between 1996 and 2005, the prevalence of underweight children fell from 56 to 45 percent, while stunting fell from 55 to 40 percent.
Moreover, Bangladesh has made impressive gains in reducing child malnutrition over the last decade; levels of malnutrition remain unusually high in comparison to other developing countries, and relative to the country’s level of per capita GDP. One in four households in Bangladesh is food insecure while two million children aged six months to five years are affected by acute malnutrition (wasting: 13.5 percent), according to a recent survey released today by WFP, UNICEF and the Institute of Public Health Nutrition (IPHN). Out of those two million malnourished children, half a million are suffering from severe acute malnutrition (severe wasting: 3.4 percent), a highly vulnerable condition where the child needs appropriate management and treatment. Given that the nationwide survey was carried out during a harvest season, the malnutrition levels are expected to be even higher during periods of food scarcity. Several surveys show that half of the children aged six months to five years are stunted (48.6 percent) – too short for their age – which depicts a very high prevalence of chronic malnutrition – one of the highest in South Asia. In addition, 37.4 percent of the same children are also underweight.
Among the causes of malnutrition, the survey identified the diet diversity as a key problem. Almost half of the children aged 6 months to 2 years – a crucial age for development – did not receive the minimum meal frequency and two thirds of the children of the same age group did not meet the minimum dietary diversity (at least four food groups per day). Not surprisingly, children in their first two years presented the highest rates of acute malnutrition. Poor infant and young child feeding practices are major factors for the nutritional situation. According to the assessment, only about one-half of mothers exclusively breastfeed children under six months and though most mothers (89 percent) continue to breastfeed their children to the recommended age of two years, complementary foods are introduced inappropriately and with insufficient dietary diversity.
It was also found that only half the mothers were aware of exclusive breast-feeding of infants for the first six months as prescribed by the World Health Organization (WHO). WFP recognizes chronic deprivation of the socially vulnerable, natural disasters and poor health services and hygiene practices as factors posing the highest threat to achieving food security, all of which are prevalent in Bangladesh.
One study was undertaken to investigate the independent effect of the length of birth interval on malnutrition in infants, and children aged 6–39 months. The survey recorded the individual weights of 1887 children. The proportion of children whose weight-for-age was below 70 percent (moderate-to-severely malnourished) and 60 percent (severely malnourished) of the NCHS median was tabulated against various durations of previous and subsequent birth intervals. Results shows that there was relation between number of older surviving siblings; maternal education and age; housing area (a proxy for wealth); age and sex of the index child; and the prevalence of diarrhoea in the previous 2 weeks for the index child.
Gender differential analysis shows that girls are more severely malnourished than the boys of same age groups. Again higher proportions of rural children are malnourished than their urban counterpart. Infant mortality decreased from 250 per 100,000 in 1962 to 94 in 1990, and 77 in 1994. Child mortality rate was 151 in 1990, which dropped to 134 in 1994. Of all the under 5 deaths, 50-60 percent were directly or indirectly related to malnutrition. More than 50 percent of all deaths in parental and neonatal period are related to low birth weight and premature delivery.
One third of all deaths among children in Bangladesh are associated with severe malnutrition. The risk of dying from severe malnutrition is high among girls compared to boys. Colostrum rejection is common (60-90 percent) in the country. Exclusive breast-feeding is only 4 percent. Bottle feeding is practiced by 90 percent mothers in urban areas. Prelacteal food is given to 100 percent of the infants. Mean weight and height of non-pregnant women are 39 kg (32-48 kg) and 148 cm (135-157 cm) respectively. Loss in mother’s body weight per child is estimated to be 1 kg. About 74 percent of adult women and 80 percent of the pregnant and lactating mothers suffer from anaemia (Hb 11g/dl blood).
JUSTIFICATION OF STUDY
Bangladesh is performing well in achieving several of the targets of health-related Millennium Development Goals (MDGs). However, there remain principal health development challenges of reducing maternal and neonatal deaths. The prevalence of malnutrition in Bangladesh is among the highest in the world. Millions of children and women suffer from one or more forms of malnutrition including low birth weight, wasting, stunting, underweight, Vitamin A deficiencies, iodine deficiency disorders and anemia. Today malnutrition not only affects individuals but its effects are passed from one generation to the next as malnourished mothers give birth to infants who struggle to develop and thrive. If these children are girls, they often grow up to become malnourished mothers themselves. Globally, malnutrition is attributed to almost one-half of all child deaths. Survivors are left vulnerable to illnesses, stunted growth and intellectual impairment.
One third of all deaths among children in Bangladesh are associated with severe malnutrition. The risk of dying from severe malnutrition is high among girls compared to boys. Poor infant and young child feeding practices are major factors for the nutritional situation. According to the assessment, only about one-half of mothers exclusively breastfeed children under six months and though most mothers (89%) continue to breastfeed their children to the recommended age of two years, complementary foods are introduced inappropriately and with insufficient dietary diversity.
Bangladeshi children also suffer from high rates of micronutrient deficiencies, particularly vitamin A, iron, iodine and zinc deficiency. Bangladesh should be commended for making significant progress in reducing vitamin A deficiency (VAD) among preschool children over the past 15 years; however, consumption of vitamin A rich foods is still low, suggesting that the underlying causes of VAD require further attention and support. Anemia is also highly prevalent among children in Bangladesh and few programs have been initiated to improve their iron status . There are different studies in the field of malnutrition and children. But most of the study conducted with the children below 5 years of age. This study considered the children below 2 years of age and the rural areas where BRAC has been working for other program not for nutrition program.
Research question
What are the factors contributing child malnutrition in rural areas in Bangladesh?
Objectives
General objective
The broad objective of this study was to assess the nutritional status of children age 6 to 24 months of the mother aged 15 and above.
Specific objectives
- To measure the nutritional status of children age 6-24 months
- To examine the relation between food habit and child nutrition
- To explore the impact of socio demographic factors on child nutrition
- To examine the effect of mother’s education on child nutrition
- To explore the relation between child diseases and nutritional status
- To see the impact of sanitation condition of the household on child nutrition
Study Design & Methods
A cross sectional descriptive study was conducted in four villages: Fulshuti, Vobukdia, Lashkordia , Talma under Nagorkanda upazilla, Faridpur district of Dhaka Division.
Sampling technique:
Non probable purposive sampling method was used for this study.
The study enrolled 127 children and their family during the study period.
Study population
The study population was the children 6 month to 24 month of the mother 15 to 35 years of age. All the mothers were selected for interview and assessing their weight and height while the children were only assessed by taking weight and height. The mothers were selected purposively who had children below 24 months.
Inclusion criteria
- Age of mother between 15 to 35 years who has child aged 6 – 24 months
- Living in the selected village
Exclusion criteria
- Mother who are above 35 years
- Unwilling to participate in the study
Data Collection, Management & Analysis
Data were collected through a structured questionnaire and checklist. Baseline information on socio-demographics, knowledge, attitude and practice with respect to maternal health and child nutrition was collected from the study participants through interviewer administered questionnaire through face to face interview. Questions were asked about mother’s age, breast feeding practice, weaning practice and any diseases of child. A check list was developed to collect information about the weight and height of the child.
Data analysis was carried out using SPSS (version 14). Categorical variables were reported as proportion, while continuous variables were reported as means and standard deviations when distributions are considered approximately normal. The chi-square test statistic was used to asses the statistical significance of the bivariate associations. T-tests were done when necessary to detect any difference between continuous variables.
Ethical consideration
Prior to the commencement of this study, the research protocol was approved by the research committee (Local Ethical committee). The aims and objectives of the study along with its procedure, risks and benefits of this study was explained to the mothers in easily understandable local language and then informed consent was taken from each mother. Then it was assured that all information and records will be kept confidential and the procedure will be used only for research purpose and the findings will be helpful for both the physician and the patients in making rational approach of the case management.
Variables
Dependent variable:
Children:
- Weight of child
- Height of child
- Any disease present during observation
- History of treatment
Maternal:
- Weight of mother
- Height of mother
- BMI of mother
- Place of delivery
- History of ANC and PNC
Independent variables:
- Age of mother
- Family income
- Education of mother
- Sanitation condition
- Mothers occupation
LITERATURE REVIEW
Malnutrition is a condition resulting from faulty, inadequate or unbalanced food. Malnutrition may also be considered as under- and over supply of nutrients than the amount needed to maintain a normal growth, development and maintenance of health. Malnutrition caused by over supply of nutrients is not a problem in Bangladesh. Rather, malnutrition caused by the under-supply of nutrients is a major public health problem in the country. A downward trend in the intake of cereals, pulses, vegetables, fruits, fish, meat, milk and oil has been recorded over last few decades. Intake of cereals has decreased from 546g in 1962-64 to 427g in 1991-92, intake of pulses decreased from 40g in 1937 to 7g in 1991-92. Similarly, vegetables intake decreased from 284g in 1937 to 176g in 1991-92. Intake of fruits, total animal foods, fish, meat, milk and oils has also decreased resulting in the decrease of intake of total amount of food.
The prevalence of malnutrition in Bangladesh is among the highest in the world. Millions of children and women suffer from one or more forms of malnutrition including low birth weight, wasting, stunting, underweight, Vitamin A deficiencies, iodine deficiency disorders and anemia. Today malnutrition not only affects individuals but its effects are passed from one generation to the next as malnourished mothers give birth to infants who struggle to develop and thrive. If these children are girls, they often grow up to become malnourished mothers themselves. Globally, malnutrition is attributed to almost one-half of all child deaths. Survivors are left vulnerable to illnesses, stunted growth and intellectual impairment.
Rates of malnutrition in Bangladesh are among the highest in the world. More than 54% of preschool-age children, equivalent to more than 9.5 million children, are stunted, 56% are underweight and more than 17% are wasted. Although all administrative divisions were affected by child malnutrition there were important differences in the prevalence of the three anthropometric indicators. The prevalence of underweight ranged from 49.8% in Khulna to 64.0% in Sylhet which also showed the highest prevalence of stunting (61.4%) and wasting (20.9%). Despite the high levels, rates of stunting have declined steadily over the past 10 years.
Bangladeshi children also suffer from high rates of micronutrient deficiencies, particularly vitamin A, iron, iodine and zinc deficiency. Bangladesh should be commended for making significant progress in reducing vitamin A deficiency (VAD) among preschool children over the past 15 years; however, consumption of vitamin A rich foods is still low, suggesting that the underlying causes of VAD require further attention and support. Anemia is also highly prevalent among children in Bangladesh and few programs have been initiated to improve their iron status.
Malnutrition among women is also extremely prevalent in Bangladesh. More than 50 percent of women suffer from chronic energy deficiency and studies suggest that there has been little improvement in women’s nutritional status over the past 20 years. As observed for children there were important differences in the prevalence of women malnutrition among administrative divisions. The prevalence of women with a BMI<18.5 kg/m2 ranged from 47.6% in Khulna to 59.6% in Sylhet. Clinical VAD is common among women of reproductive age and during pregnancy. Sub-clinical VAD and anemia are also highly prevalent among pregnant and lactating women. Programs in Bangladesh also need to begin to incorporate components for adolescents and school-age children who will also benefit from improvements in nutrition (http://www.fao.org/ag/agn/nutrition/bgd_en.stm).
The nutritional status of under five children is a sensitive indicator of a country’s health status as well as economic condition. This study investigated differential impact of some demographic, socioeconomic, environmental and health related factors on nutritional status among under five children in Bangladesh. The analyses revealed that 45 percent of the children under age five were suffering from chronic malnutrition, 10.5 percent were acutely malnourished and 48 percent had under-weight problem. The main contributing factors for under five malnutrition were found to be previous birth interval, size at birth, mother’s body mass index at birth and parent’s education (Rayhan et al. 2006).
This study was undertaken to investigate the independent effect of the length of birth interval on malnutrition in infants, and children aged 6–39 months. Data for this study were drawn from a post-flood survey conducted during October–December 1988 at Sirajganj of the Sirajgani district and at Gopalpur of the Tangail district in Bangladesh. The survey recorded the individual weights of 1887 children. Cross-tabulations and logistic regression procedures were applied to analyse the data. The proportion of children whose weight-for-age was below 70% (moderate-to-severely malnourished) and 60% (severely malnourished) of the NCHS median was tabulated against various durations of previous and subsequent birth intervals. The odds of being moderately or severely malnourished were computed for various birth intervals, controlling for: the number of older surviving siblings; maternal education and age; housing area (a proxy for wealth); age and sex of the index child; and the prevalence of diarrhea in the previous 2 weeks for the index child.
About one-third of infants and young children were moderately malnourished and 15% were severely malnourished. The proportion of children who were under 60% weight-for-age decreased with the increase in the length of the subsequent birth interval, maternal education and housing area. The proportion of malnourished children increased with the number of older surviving children. Children were at higher risk of malnutrition if they were female, their mothers were less educated, they had several siblings, and either previous or subsequent siblings were born within 24 months. This study indicates the potential importance of longer birth intervals in reducing malnutrition in children (Mozumder et al. 2000).
Study examined whether malnutrition increased the risk of diarrhea equally for all enteropathogens. The study was conducted prospectively between January 1999 and July 2002 in Mirpur, an urban slum in Dhaka. Two hundred eighty-nine Bangladeshi children (147 male and 142 female) 2–5 years of age were included in the study. Malnutrition was present in 39% of the children at the time of enrollment. Of the identified enteropathogens, only enterotoxigenic Escherichia coli (ETEC), Cryptosporidium sp., and Entamoeba histolytica were significantly more prevalent in malnourished children. We concluded that the malnutrition attributed risk is not equal for enteric pathogens associated with diarrheal illness (Mondal et al. 2009).
As a result of low intake of nutrients, lack of nutrition education, food taboos, traditional food habits, excessive and unscientific methods of processing and cooking, faulty intra-household food distribution among the members of the family, large-scale adulteration of foods, infection and frequent attack of diarrhoeal diseases, measles, partussis, faulty weaning practices, and for some other related causes, the nutritional status of the people is very poor.
Most affected group of population is the children and the pregnant and lactating mothers. Only 6.2% of the children aged 0-72 months are normal. The remaining 93.8% children suffer from various degrees of malnutrition.
Maternal mortality is as high as 450 per 100,000. Mean birth weight of babies is 2.7 kg, 37-41% babies born in rural areas are of low birth weight (2500g) as against 23-27% babies in urban areas. About 1.7% of the children aged between 6 and 71 months in 1989 suffered from night blindness compared to 3.6% in 1982-83, and about 30,000 children are becoming blind every year due to vitamin A deficiency. The people of Bangladesh are at a risk of iodine deficiency. In 2000, about 69% of the population were iodine deficient, 47% had goitre and 9% had visible goitre, about 5,00,000 persons were mentally retarded due to iodine deficiency
Gender differential analysis shows that girls are more severely malnourished than the boys of same age groups. Again higher proportions of rural children are malnourished than their urban counterpart. Infant mortality decreased from 250 per 100,000 in 1962 to 94 in 1990, and 77 in 1994. Child mortality rate was 151 in 1990, which dropped to 134 in 1994. Of all the under 5 deaths, 50-60% were directly or indirectly related to malnutrition. More than 50% of all deaths in parental and neonatal period are related to low birth weight and premature delivery (Mondal et al. 2009).
One third of all deaths among children in Bangladesh is associated with severe malnutrition. The risk of dying from severe malnutrition is high among girls compared to boys. Colostrum rejection is common (60-90%) in the country. Exclusive breast-feeding is only 4%. Bottle feeding is practiced by 90% mothers in urban areas. Prelacteal food is given to 100% of the infants. Mean weight and height of non-pregnant women are 39 kg (32-48 kg) and 148 cm (135-157 cm) respectively. Loss in mother’s body weight per child is estimated to be 1 kg. About 74% of adult women and 80% of the pregnant and lactating mothers suffer from anemia
Although the country has recently achieved nearly self-sufficiency in food production that is, mainly rice and to a lesser extent wheat, the poor children have little access to the food because of lack of buying capacity on the part of their parents. Also, rice alone cannot provide the necessary nutrients for balanced growth; there is a need for certain amount of protein intake such as meat and fish, and of food items with high vitamin and mineral content such as fruits and vegetables. The typical manifestation of child malnutrition is a deficiency what is described as protein-energy malnutrition – that is, deficiency of both protein-containing food and energy-providing cereal. Prolonged protein-energy malnutrition in children results in growth stunting and wasting; weight gained at a certain age (weight for age) is much less than what is accepted as normal in such children.
In the mid-1990s, it was estimated by the FAO that about 56% of Bangladesh’s children were underweight for their age suggesting chronic malnutrition. The situation has not improved. Around two-thirds of children under the age of five years suffer from some degree of malnutrition in Bangladesh. Malnourished children are more vulnerable to infectious diseases, have stunted growth and suffer from slower mental development. Data show that with per capita annual income of less than Tk 2,000, nearly 85% of the children in that income-group are malnourished. With per capita annual income in the range Tk 2,000 to 10,000 about 60% children are malnourished, and with over Tk 12,000 the percentage of malnourished children is still quite high, about 30%. The last finding suggests that only income is not sufficient for achieving proper nutritional status, there are other factors such as food habit, disease susceptibility etc that are also to be taken into account.
An NGO called Hunger Project recently (end of year 2000) estimated that in Bangladesh as many as 700 deaths occur in a day, of which 655 are children, due to causes related to ‘persistent hunger’. This is an astounding figure, but given the level of acute poverty and its painful manifestations that are too seen in various settings, the figures may not be too far removed from the truth. This nutritional deprivation occurred despite many of the nutritional intervention programmes that were instituted by the government under the aegis of the World Bank to cushion the adverse effects of free market transition on health of the poor. Among these, a major project was the National Integrated Nutrition Project, funded by the World Bank, and Vulnerable Group Feeding programme. These were targeted at the poor below poverty line, since it is well established that this group suffers most for a few years during the transition from a regulated economy to free market economy; these people become poorer during this time with grave consequences on their nutritional status.
Child malnutrition due to vitamin A deficiency that causes night-blindness in children is high in Bangladesh. Most rural children run a high risk of vitamin A deficiency because of inadequate dietary intake of the vitamin, due largely to poverty, and partly due to poor eating habits resulting from ignorance. Surveys that have been carried out in recent years suggest a prevalence of vitamin A-associated night blindness in children of 1-6 years of age, of about 2%. Each day, nearly 82 children become blind in Bangladesh due to vitamin A deficiency, again an unbelievable number, but it tells the painful truth. For infants, it has been found that the Bangladeshi lactating mother can provide nearly 70% of the infant’s vitamin A requirement. Vegetables and fruits are very rich in vitamin A. Homesteads in rural areas can serve well in producing green vegetables for the family with little cost and effort in our country since the weather is congenial for cultivation of some vegetables and fruits throughout the year. In recent years the government has instituted the EPI programme where children under the age of 5 years are given high potency vitamin A capsule. However, the coverage achieved so far varies considerably from region to region, the range is 16% to 85%.
Another nutritional deficiency in children of Bangladesh is iodine deficiency disorder (IDD). But the problem is more pronounced among the adults. To ameliorate this, the government has promoted production and marketing of iodized salt which, it is hoped, will largely eliminate this deficiency from the population
One study conducted by Azizur Rahman and his team revealed that the prevalence of severeand moderate wasting were more common among children, and theoverall prevalence of acute malnutrition was about 10%, indicatingthat it is one of the major public health problems in the country.Multivariate analysis showed that mother’s BMI and media exposure,child’s age and birth size, and respiratory sickness in childhoodwere significantly associated with both severe and moderatewasting (Rahman,2009).
As a result of inappropriate feeding, poor health and hygiene, and poor caring practices, the nutritional status of many young infants deteriorates with advancing age. One study conducted by Roy and his team to explore the effectiveness of a nutrition education package to prevent malnutrition among young children. A community-based, randomized, controlled trial was conducted among 605 normal and mildly malnourished children aged 6 to 9 months in 121 Community Nutrition Centers (CNCs) of the Bangladesh Integrated Nutrition Project (BINP) in four regions of Bangladesh from 2000 to 2002. The intervention group received weekly nutrition education based on the nutrition triangle concept of UNICEF for 6 months, whereas the control group received regular BINP services. Both groups were observed for a further 6 months to assess the sustainability of the effects. Information on socioeconomic status, feeding patterns, morbidity, and anthropometric features was collected. Study findings revealed that a significant increase in the frequency of complementary feeding was observed in the intervention group as compared with the control group, and the increase was sustained throughout the observation period. The intervention group had a higher weight gain than the control group after the end of the intervention (0.86 vs. 0.77 kg, p = 0.053) and after the end of the observation period (1.81 vs. 1.39 kg, p < .001). The proportion of normal and mildly malnourished children was greater in the intervention group than in the control group after the end of the observations (88.9% vs. 61.5%, p < .001). Nutrition education successfully prevented malnutrition in all the areas. Variation in the outcome of nutrition education among the regions was observed. This culturally appropriate nutrition education package based on the nutrition triangle model effectively prevented growth faltering and malnutrition among young children (Roy 2007).
Children are tomorrow’s world or tomorrow’s father” this slogan is riding a massive wave of concern throughout the world. But children, all over the world are deprived of many facilities. Hunger and malnutrition make them worst sufferers and these pose potential threats to mankind as a whole or to the civilization itself. The children of Bangladesh are particularly more victimized than those in other part of the world1. Although there has been a steady decline in the infant mortality rate in Bangladesh (87 per thousand live births in 1993-1994 to 65 per thousand in 2004) but overall health condition and nutritional status of children is not so well (Alnda 2008).
The nutritional status of under-five children is of particular concern, since the early years of life are crucial for future growth and development. Globally, nutritional status is considered the best indicator of the well being of young children and a parameter for monitoring progress towards the Millennium Development Goals (MDGs), especially MDG1 (Semba 2008). In developing countries, an estimated 50.6 million children aged less than five years are malnourished4. Low birth weight (<2,500g) is an especially important indicator: both as a marker of overall health of the mother and as a predictor of ill health for newborns. Poor nutrition severely hinders personal, social and national development5. Bangladesh has the highest prevalence of childhood underweight among all countries in the world, except North Korea, and only seven countries have a higher prevalence of child stunting. Rates of low birth weight among Bangladeshi children are among the highest in the world with 20-40% of babies weighting less than 2,500g at birth. It has been though that improved nutrition for mothers during pregnancy would reduce this rate (Faruque 2008). The percentage of children aged 6-59 months with stunting decreased from 64.2% in 1992 to 48.3% in 2000 and 42.4% in 2005, under weight decreased from 68.3% in 1992 to 51.0% in 2000 and 47.8% in 2005, and wasting decreased from 16.7% in 1992 to 12.0% in 2000 and remained at 12.7% in 2005 (Mosiur Rahman 2009; BSS 2007).
The interactions between malnutrition and infection are mutually adverse. The results of these interactions are of public health importance in developing countries where malnutrition and infection often co-exist. Recent studies highlight the mechanisms involved in these interactions and indicate the necessity for a comprehensive approach to control malnutrition in poor communities.
Diarrhea and malnutrition are common in young children in developing countries and a reciprocal relationship has been postulated with diarrhea leading to malnutrition and malnutrition predisposing to diarrhea. To investigate the importance of malnutrition as a determining factor in diarrheal illnesses, data were analyzed from a longitudinal community-based study done in rural Bangladesh. Children classified by nutritional status according to a variety of anthropometric indicators were prospectively evaluated for incidence, duration, and etiology of diarrhea. Children with low weight for length had longer durations of diarrhea than better nourished children; however, children of differing nutritional status had similar diarrheal incidences. The duration of diarrhea, including that associated with enterotoxigenic Escherichia coli and Shigella, increased progressively as nutritional status indicators worsened. These results suggest that nutritional interventions alone are unlikely to reduce the high incidence of diarrhea, but that efforts to improve nutritional status may have a beneficial effect on the duration of diarrhea and its unfavorable nutritional consequences (Black 1984).
Similar type of study was conducted by Bairagi. They explored the interaction between diarrhoeal disease and nutritional status measured by anthropometry was investigated in approximately 1000 children aged 1 to 4 years during April-December 1976 in a rural area of Bangladesh. Data on diarrhoeal disease were provided by the mothers interviewed at seven-day intervals. Weight and height data were collected bimonthly. Children classified using anthropometric criteria—weight-for-age, height-for-age, and weight-for-height—were prospectively evaluated for incidence and duration of diarrhoea during a short (two-month) period and a long (eight-month) period. Incidence of diarrhoea was not found to be related to nutritional status measured by any of the anthropometric criteria for any of the periods. But duration of diarrhoea was found to be related consistently to nutritional status measured by weight-for-age and weight-for-height. Diarrhoea in the short term affected weight increment in the short term, but not in the long term and did not affect height increment for any of these periods. Diarrhoea in the long term affected both weight increment and height increment in the long term (Bairagi et al. 1987).
Dewan and the team also found the same result in their study. Study findings revealed that compared to non diarrhoea and non dysentery diarrhea was associated with significantly lower annual weight gain. Both 3-month dysentery and non-dysentery intervals were significantly associated with less weight gain compared to non-diarrhoea intervals. Dysentery intervals were also associated with significantly poorer height gain compared to other intervals. The growth of young children is strongly influenced by the clinical type of diarrhoea and the impact is dependent on the proportion of dysentery episodes in the total diarrhoeal burden (Dewan 2000).
RESULTS
The children who were assessed for weight and height among them 54 percent were male and 46 percent were female. The ratio of male and female was 1.15: 1
Distribution of the children by sex
| Sex of the children | Frequency | Percent |
| Male | 68 | 53.5 |
| Female | 59 | 46.5 |
| Total | 127 | 100.0 |
the age distribution of the children. The children who were assessed in the study, among them around 30 percent were 6-11 months and another 30 percent were 12-17 months and remaining 40 percent were 18-24 months.
Distribution of the children by age
| Age of the children | Frequency | Percent |
| 6-11 months | 38 | 29.9 |
| 12-17 months | 38 | 29.9 |
| 18-23 months | 51 | 40.2 |
| Total | 127 | 100.0 |
| Mean ± SD (Range) | 15.82 ± 5.52 | 6.1-23.9 |
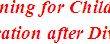
the age distribution by sex of the children who were participated in the study. Among the male children 35.3 percent were between ages 6-11 months, 22.1 percent were 12-17 months and remaining 43.6 percent were between 18-24 months. Similarly, among the female children, 23.7 percent were between ages 6-11 months, 39 percent were 12-17 months and remaining 37.3 percent were between 18-24 months. It is observed that there is variation in age group among the male and female children.
Distribution of the children age by sex
Mothers of the assessed children also asked about the delivery history of their last child. About 70 percent women informed that they delivered their child at home while 14 percent deliveries were taken place in government hospital and 16 percent in private clinics. Findings suggest that still home delivery is predominant among the rural women (Fig. 2).
Bar diagram of the children by place of delivery
the delivery conducted by different personnel. Mothers of the assessed children also asked about the delivery history of their last child. They were requested to inform who conducted the delivery. According to the findings, it was observed that about 42 percent deliveries were conducted by trained Traditional Birth Attendants (TBA) 31 percent by trained midwife and 24 percent by untrained Traditional Birth Attendants (TBA) attendants. And remaining percent of deliveries was conducted by family members. Although a large percentage of deliveries conducted by trained personnel but still a significant percentage of deliveries are conducted by untrained personnel.
Distribution of the children by who conducted delivery
| Who conducted delivery | Frequency | Percent |
| Trained TBA | 54 | 42.5 |
| Trained midwife | 40 | 31.5 |
| Non trained TBA | 31 | 24.4 |
| Family TBA | 2 | 1.6 |
| Total | 127 | 100.0 |
the gestational age distribution of children who were participated in the study. Study findings shows that majority of the children delivered within 38-40 weeks of gestational age. Only three percent delivered before completion of 37 weeks.
Distribution of the children by gestational age (in weeks)
| Gestational age | Frequency | Percent |
| ≤37 weeks | 4 | 3.1 |
| 38-40 weeks | 122 | 96.1 |
| >40 weeks | 1 | .8 |
| Total | 127 | 100.0 |
Mothers of assessed children were asked about the colostrums feeding just after birth. Table 5 shows the percent distribution of children by colostrums feeding after birth. Data shows that more than 95 percent mothers fed colostrums their babies after birth which indicates a higher knowledge about colostrums feeding after birth.
istribution of the children by colostrums feeding after birth
| Colostrums feeding after birth | Frequency | Percent |
| Yes | 120 | 94.5 |
| No | 7 | 5.5 |
| Total | 127 | 100.0 |
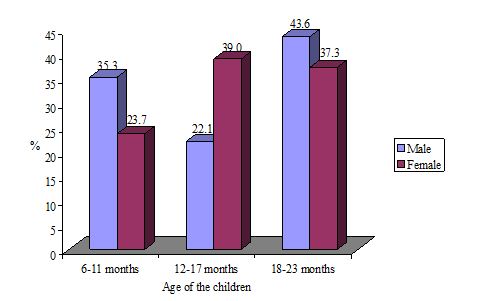
Detailed information was collected from the mothers about their feeding practice after birth of their assessed babies. Fig. 3 shows the distribution of children by pre-lacteal feeding after birth. Findings suggest that a significant percentage of mother fed breast milk to their newborn babies after birth while 15 percent of mothers fed honey before breast milk. It was also observed that a few percentage of mothers also fed powder milk, cow milk and other food to child after birth as the substitute of breast milk.
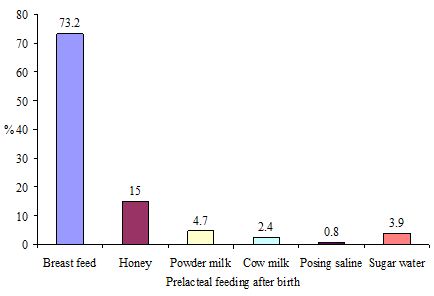
Figure Bar diagram of the children by prelacteal feeding after birth
Information regarding weaning practice of mother was collected. the distribution of children by their first weaning food practice. Findings suggest that majority of the mother started their weaning practice for the child with cow milk followed by powder milk. Very negligible percentage of mother mentioned fruit juice, paish (rice base sweet), rice, khichuri, sagu etc. Although khichuri is a very nutritious food as for children who above five years but most of the mothers practice other khichuri.
Distribution of the children by first weaning food practice
| First weaning food practice | Frequency | Percent |
| Cow milk | 78 | 61.4 |
| Power milk | 22 | 17.3 |
| Fruit juice | 8 | 6.3 |
| Paish | 2 | 1.6 |
| Khicuri | 3 | 2.4 |
| Rice | 2 | 1.6 |
| Sagu | 1 | .8 |
| Egg | 4 | 3.1 |
| Sugi | 1 | .8 |
| Biscuit | 2 | 1.6 |
| Others | 4 | 3.1 |
| Total | 127 | 100.0 |
the detail information of food practice of assessed children provided by family members in 24 hours collected from the the mothers. Findings suggest that carbohydrate (sugi, rice, khichuri etc) was the dominant regular food for children as daily food provided by mothers followed by cow milk. Mothers also informed that they provide protein like fish, egg and milk in their daily food to their babies. Findings suggest that there is mix practice in food habit for the children who are under 24 months.
Distribution of the children by CF practice in 24 hours recall
| CF practice in 24 hours recall | Frequency | Percent |
| Milk | 83 | 65.4 |
| Protein | 41 | 32.3 |
| Carbohydrate | 117 | 92.1 |
Multiple responses
Immunization is an important indicators for the children for their good health care practice. Detailed information was collected from the mothers about the immunization of their children. They were also asked to show the immunization card. Findings suggest that 87.6 percent children completed their immunization while 12.4 percent did not. It may be due to age of the children because some children were bellow 9 months (Table 8).
Distribution of the children by EPI in age between 1 to 2 years
| EPI | Frequency | Percent |
| Complete | 78 | 87.6 |
| Incomplete | 11 | 12.4 |
| Total | 89 | 100.0 |
the distribution of the children by Vit-A intake who were above 1 year of age. Vitamin A campaign is a major activity of DGHS of Bangladesh government for all under five children to reduce vitamin deficiency malnutrition. Information regarding Vit-A intake was collected from the mothers. Findings suggest that 83.1 percent children were under Vit-A campaign while only 16.9 percent children were not. This percentage may be due to below age of 1 year.
Distribution of the children by Vitamin-A in age between 1 to 2 years
| Vitamin-A | Frequency | Percent |
| Yes | 74 | 83.1 |
| No | 15 | 16.9 |
| Total | 89 | 100.0 |
distribution of the children by disease during the last15 days. All the mothers who participated in the study were asked about the diseases history of their children during the last15 days. About 57 percent mothers reported that their child suffered from various diseases during last three months. Remaining 43 percents did not have any history of diseases during the same period.
Distribution of the children by disease during last 15 day
| Presence of diseases | Frequency | Percent |
| Yes | 72 | 56.7 |
| No | 55 | 43.3 |
| Total | 127 | 100.0 |
distribution of the children by types of diseases within last 15 days. A significant percentage of mothers reported that their children suffered from diarrhea and dysentery followed by common cold and fever. A few percentages of children also suffered from other diseases like pneumonia, skin disease and measles.
Distribution of the children by type of diseases within 15 days
| Type of diseases* | Frequency | Percent |
| Fever | 18 | 25.0 |
| Common cold | 24 | 33.3 |
| Diarrhea | 28 | 38.9 |
| Pneumonia | 1 | 1.4 |
| Dysentery | 8 | 11.1 |
| Vomiting | 3 | 4.2 |
| Skin disease | 4 | 5.6 |
| Measles | 2 | 2.8 |
*Multiple responses
distribution of the children by whom they were during their illness during last 15 days of survey. A significant percentage of mothers reported that their children suffered from diarrhea and dysentery followed by common cold and fever. A few percentages of children also suffered from other diseases like pneumonia, skin disease and measles. Public facilities like H&FWCs, UHCs and district hospitals (41.7 percent) were the major sources of services informed by the mothers followed by village doctors (36.2 percent) who are unqualified. Other sources of providers also were private doctors which are about 11 percent. About 11 percent mothers sought services from other different sources.
Distribution of the children by who treated these patients
| Who treated these patients | Frequency | Percent |
| Govt. hospital | 53 | 41.7 |
| Clinic | 2 | 1.6 |
| Private doctor | 14 | 11.0 |
| Village doctor | 46 | 36.2 |
| Others | 12 | 9.4 |
| Total | 127 | 100.0 |
distribution of mother by their age. The mothers who were participated in the study were 15 years to 35 years. Majority of the mothers were above 20 years, among them 37.8 percent were 20-24 years, 24.4 percent were between 25-29 years and 26.8 percent were 30 or above 30 years.
Distribution of mother by age
| Age of mother | Frequency | Percent |
| <20 | 14 | 11.0 |
| 20-24 | 48 | 37.8 |
| 25-29 | 31 | 24.4 |
| ≥30 | 34 | 26.8 |
| Total | 127 | 100.0 |
| Mean ± SD (Range) | 25.13 ± 5.26 | (18-40) |
distribution of mother by occupation. The mothers who were participated in the study were mostly housewife while only 2.4 percent mothers were service holders.
Distribution of mother by occupation
| Occupation of mother | Frequency | Percent |
| Housewife | 124 | 97.6 |
| Service | 3 | 2.4 |
| Total | 127 | 100.0 |
the distribution of house quality of the study household. All the households were assessed whether the houses were constructed or paka or other quality like tin, wood, mati or bera. Findings shows that majority of the houses (83.5 percent) were made in tin and remaining 16.5 percent houses made by other materials.
Distribution of house quality
| House quality | Frequency | Percent |
| Paka | 4 | 3.1 |
| Semi paka | 11 | 8.7 |
| Tin | 106 | 83.5 |
| Wood | 2 | 1.6 |
| Mati | 1 | .8 |
| Bera | 3 | 2.4 |
| Total | 127 | 100.0 |
the distribution of sanitation condition of the study household. Saniatation facilities of all the households were observed whether the houses were paka, ring slab, kacha or open. Findings shows that 73.2 percent household had ring slab sanitation facilities while 14.2 percent had paka sanitation facilities and remaining 12.6 percent households had kacha or open sanitation facilities.
Distribution of sanitation
| Sanitation | Frequency | Percent |
| Paka | 18 | 14.2 |
| Ring slab | 93 | 73.2 |
| Kacha | 7 | 5.5 |
| Open | 9 | 7.1 |
| Total | 127 | 100.0 |
the distribution of family income of the study household. Findings show that 51.2 percent household had income below 5,000 while 39.4 percent families had income between 5,000-10,000. Only 9.4 percent families had income above 10,000 taka.
Distribution of family income
| Family income | Frequency | Percent |
| ≤5000 | 65 | 51.2 |
| 5001-10000 | 50 | 39.4 |
| >10000 | 12 | 9.4 |
| Total | 127 | 100.0 |
| Mean ± SD (Range) | 6858.66 ± 5126.11 | (1500.00-35000.00) |
The distribution of the children by weight. All the children weighted. Findings show that a significant percentage of children were less than 10 kg (81.1 percent) while 18.9 percent were above 10 kg.
Table : Distribution of the children by weight
| Weight (in KG) | Frequency | Percent |
| ≤10 | 103 | 81.1 |
| >10 | 24 | 18.9 |
| Total | 127 | 100.0 |
| Mean ± SD (Range) | 8.65 ± 1.47 | (5.3-14.0) |
The distribution of the children by height. The height was measured for all the children. Findings show that 29.9 percent of children were less than 70 cm, while 63 percent were between 70-80cm and only 7.1 above 80 cm.
Table : Distribution of the children by height
| Height (in cm) | Frequency | Percent |
| ≤70 | 38 | 29.9 |
| 70-80 | 80 | 63.0 |
| >80 | 9 | 7.1 |
| Total | 127 | 100.0 |
| Mean ± SD (Range) | 73.69 ± 5.49 | (62-88) |
Table : Distribution of children malnutrition by sex
| Malnutrition | Sex of children | Total | |
Male (n=68) | Female (n=59) | ||
| Underweight | 29 (42.6) # | 19 (32.2) | 48 (37.8) |
| Stunting | 33 (48.5) | 23 (39.0) | 56 (44.1) |
| Wasting | 11 (16.2) | 8 (13.6) | 19 (15.0) |
The distribution of the children malnutrition by age. Findings show that among 127 children, 23.7 percent children who were within age 6 month to 11 months were underweight while it was 42.1 percent for the age group 12 months to 17 months. Similarly, 45.1 percent children age 18 months to 23 months were underweight. The tendency of underweight increased with age. In case of stunting, 31.6 percent children who were within age 6 month to 11 months were stunting while it was 36.8 percent for the age group 12 months to 17 months. Similarly, 58.8 percent children age 18 months to 23 months were stunting. The similar relationship was observed regarding underweight and stunting and the age. For the case of wasting a different situation was observed. Twenty one percent children who were within age 6 month to 11 months were suffering from wasting while it was 7.9 percent for the age group 12 months to 17 months. Similarly, 15.7 percent children age 18 months to 23 months were suffering from wasting.
Table : Distribution of children malnutrition by age
| Malnutrition | Age of children | Total | ||
6-11 months (n=38) | 12-17 months (n=38) | 18-23 months (n=51) | ||
| Underweight | 9 (23.7) # | 16 (42.1) | 23 (45.1) | 48(37.8) |
| Stunting | 12 (31.6) | 14 (36.8) | 30 (58.8) | 56(44.1) |
| Wasting | 8 (21.1) | 3 (7.9) | 8 (15.7) | 19(15.0) |
The distribution of the children malnutrition by presence of diseases. Findings show that the children who suffered from fever among them, 70.6 percent were underweight, 70.6 percent were stunting and 17.6 percent were wasting. Similarly, children who suffered from common cold and other respiratory diseases among them, 50 percent were underweight, 45.8 percent were stunting and 25 percent were wasting. It was also observed that children who suffered from diarrhea among them, 28.6 percent were underweight, 25 percent were stunting and 14.3 percent were wasting. It is important to note that the children who suffered from fever during the last 15 days of survey period were more likely to develop malnutrition followed by respiratory diseases and diarrhea.
The distribution of the children malnutrition by age of mother. Findings show that there were only 14 mothers who were below 20 years of age. It was observed that 28.6 percent of the total children of the mother of age below 20 years were underweight while 57.1 percent were stunting and 7.1 percent were wasting. Among 127 children, 33.3 percent children whom mothers were aged between 20-24 years were underweight while it was 37.5 for stunting and 14.6 were wasting. Similar findings also were observed among the children whom mothers were aged between 25-30 years except for the cases of wasting which was higher among the children of mothers aged 25-30 years. Important findings observed among the children whom mothers were above 30 years of age. Fifty percent of the children were underweight; 58.8 percent children were stunting and 29.4 percent children were wasting whom mothers were above 30 years of age.
Table : Distribution of children malnutrition by age of mother
| Malnutrition | Age of mother (in year) | Total | |||
<20 (n=14) | 20-24 (n=48) | 25-30 (n=31) | >=30 (n=34) | ||
| Underweight | 4(28.6# | 16 (33.3) | 11 (35.5) | 17 (50.0) | 48 (37.8) |
| Stunting | 8(57.1) | 18 (37.5) | 10 (32.3) | 20 (58.8) | 56 (44.1) |
| Wasting | 1 (7.1) | 7 (14.6) | 1 (3.2) | 10 (29.4) | 19 (15.0) |
Figure within parentheses indicates in column percentage.
The distribution of the children malnutrition by education of mother. Findings show that there were significant differences among the children by their nutritional status according their mother’s education. It was observed that higher number of children suffered from malnutrition that mothers were illiterate. Forty nine percent children suffered from underweight; 66.7 percent suffered from stunting and 17.6 percent suffered from wasting among the total children and their mothers were illiterate. Similarly, 35.5 percent children suffered from underweight; 33.9 percent suffered from stunting and 12.9 percent children suffered from wasting among the total children and their mothers had primary education. Nutritional level was better among the children of mothers with secondary education.
Table : Distribution of children malnutrition by education of mother
| Malnutrition | Education of mother | Total | |||
Illiterate (n=51) | Primary (n=62) | Secondary (n=6) | Higher secondary and above (n=8) | ||
| Underweight | 25 (49.0)# | 22 (35.5) | 0 (.0) | 1 (12.5) | 48 (37.8) |
| Stunting | 34 (66.7) | 21 (33.9) | 0 (.0) | 1 (12.5) | 56 (44.1) |
| Wasting | 9 (17.6) | 8 (12.9) | 1 (16.7) | 1 (12.5) | 19 (15.0) |
Figure within parentheses indicates in column percentage.
Table: Distribution of children malnutrition by monthly family income
| Malnutrition | Monthly family income (in taka) | Total | ||
≤5000 (n=65) | 5001-10000 (n=50) | >10000 (n=12) | ||
| Underweight | 26 (40.0) # | 20 (40.0) | 2 (16.7) | 48 (37.8) |
| Stunting | 34 (52.3) | 21 (42.0) | 1 (8.3) | 56 (44.1) |
| Wasting | 11 (16.9) | 6 (12.0) | 2 (16.7) | 19 (15.0) |
Figure within parentheses indicates in column percentage.
The distribution of the children malnutrition by family income. Findings show that there were significant differences among the children by their family income. It was observed that higher number of children suffered from malnutrition whom family income was lower. Forty percent children were underweight; 52.3 percent were stunted and 16.9 percent suffered from wasting among the total children and their family income was 5000 taka or below. Similarly, 40 percent children suffered from underweight; 42.0 percent suffered from stunting and 12.0 percent children suffered from wasting among the total children and their family income was between 5000-10000 taka per month. Improved situation was observed among the children whom family income was above 10000 taka per month.
DISCUSSION
Over the past two decades Bangladesh has made impressive gain in key health indicators, which are important to achieve maternal and child health-related MDGs 4 and 5 (NIPORT, Mitra and Associates, and Macro International 2008). From 1989 to 2007, maternal mortality ratio (MMR) declined from 650 to 322 per 100,000 live births, and under-five child mortality rate dropped from 133 to 65 per 1,000 live births. However, MMR in Bangladesh is still one of the highest in the world; and Bangladesh is still far away from achieving the MDG target of reducing MMR to 143 by the year 2015 (ICDDR,B 2007). Encouragingly, Bangladesh is considered to be on track in reducing child mortality rate but sustaining this rate will demand cautious and continued effort (ICDDR,B 2007; Mitra et al. 1994; NIPORT, ORC Macro, Johns Hopkins University, and ICDDR,B 2003; NIPORT, Mitra and Associates, and Macro International 2008). Inequalities in terms of socio-economic status, low access to health services, inequalities in economic development and geographic location are major challenges in achieving equitable development in maternal and child health (Islam 2008; NIPORT, Mitra and Associates, and Macro International 2008).
However, between 1996 and 2005, the prevalence of underweight children fell from 56 to 45 percent, while stunting fell from 55 to 40 percent. Moreover, Bangladesh has made impressive gains in reducing child malnutrition over the last decade; levels of malnutrition remain unusually high in comparison to other developing countries, and relative to the country’s level of per capita GDP. One in four households in Bangladesh is food insecure while two million children aged six months to five years are affected by acute malnutrition (wasting: 13.5%), according to a recent survey released today by WFP, UNICEF and the Institute of Public Health Nutrition (IPHN). Out of those two million malnourished children, half a million are suffering from severe acute malnutrition (severe wasting: 3.4%), a highly vulnerable condition where the child needs appropriate management and treatment. Given that the nationwide survey was carried out during a harvest season, the malnutrition levels are expected to be even higher during periods of food scarcity. Several surveys show that half of the children aged six months to five years are stunted (48.6%) – too short for their age – which depicts a very high prevalence of chronic malnutrition – one of the highest in South Asia. In addition, 37.4% of the same children are also underweight.
The study was conducted in four rural villages to see the nutritional status of children below two years of age and their mother’s age was between 15 to 35 years. There were diversifications in occupation of the household head. Findings show that similar proportions of the household heads were farmer, businessman and service holders. About 10 and 5.5 percent head of households was rickshaw puller, driver respectively. Remaining 11 percent household heads were involved in different activities in different time.Findings show that 51.2 percent household had income below 5,000 while 39.4 percent families had income between 5,000-10,000 taka. Only 9.4 percent families had income above 10,000 taka.
All the mother who participated in the study were asked whether they are involved any organization like NGO group, women group, samitte etc. Findings shows that a significant percentage of mothers were involved in different organizations (70 percent) while, about 30 percent were not involved in any organization.
Findings
Findings shows that majority of the houses (83.5 percent) were made in tin and remaining 16.5 percent houses made by other materials. Saniatation facilities of all the households were observed whether the houses were paka, ring slab, kacha or open. Findings shows that 73.2 percent household had ring slab sanitation facilities while 14.2 percent had paka sanitation facilities and remaining 12.6 percent households had kacha or open saniation facilities.
The children who were assessed for weight and height among them 54 percent were male and 46 percent were female. The ratio of male and female was 1.15: 1. The children who were assessed in the study, among them around 30 percent were 6-11 months and another 30 percent were 12-17 months and remaining 40 percent were 18-24 months. Among the male children 35.3 percent were between ages 6-11 months, 22.1 percent were 12-17 months and remaining 43.6 percent were between 18-24 months. Similarly, among the female children, 23.7 percent were between ages 6-11 months, 39 percent were 12-17 months and remaining 37.3 percent were between 18-24 months. About 70 percent deliveries were taken place at home while 14 percent in government hospital and 16 percent in private clinics. Findings suggest that still home delivery is predominant among the rural women. According to the findings, it was observed that about 42 percent deliveries were conducted by trained TBA, 31 percent by trained midwife and 24 percent by untrained TBA. And remaining percent of deliveries was conducted by family members. Although a large percentage of deliveries conducted by trained personnel but still a significant percentage of deliveries are conducted by untrained personnel. Study findings shows that majority of the children delivered within 38-40 weeks of gestational age. Only three percent delivered before completion of 37 weeks. Data shows that more than 95 percent mothers fed colostrums their babies after birth which indicates a higher knowledge about colostrums feeding after birth. Findings suggest that a significant percentage of mother fed breast milk to their newborn babies after birth while 15 percent of mothers fed honey before breast milk. It was also observed that a few percentage of mothers also fed powder milk, cow milk and other food to child after birth as the substitute of breast milk. It was observed that majority of the mother started their weaning practice for the child with cow milk followed by powder milk. Very negligible percentage of mother mentioned fruit juice, paish (rice base sweet), rice, khichuri, sagu etc. Although khichuri is a very nutritious food as for children who above five years but most of the mothers practice other khichuri.
Findings suggest that carbohydrate (sugi, rice, khichuri etc) was the dominant regular food for children as daily food provided by mothers followed by cow milk. Mothers also informed that they provide protein like fish, egg and milk in their daily food to their babies. Findings suggest that there is mix practice in food habit for the children who are under 24 months. Immunization is an important indicator for the children for their good health care practice. Findings suggest that 87.6 percent children completed their immunization while 12.4 percent did not.Vitamin A campaign is a major activity of DGHS of Bangladesh government for all under five children to reduce vitamin deficiency malnutrition. Findings suggest that 83.1 percent children were under Vit-A campaign while only 16.9 percent children were not. About 57 percent mothers reported that their child suffered from various diseases during last 15 days. Remaining 43 percents did not have any history of diseases during the same period. Public facilities like H&FWCs, UHCs and district hospitals (41.7 percent) were the major sources of services informed by the mothers followed by village doctors (36.2 percent) who are unqualified. Other sources of providers also were private doctors which are about 11 percent. About 11 percent mothers sought services from other different sources.
The mothers who were participated in the study were 15 years to 35 years. Majority of the mothers were above 20 years, among them 37.8 percent were 20-24 years, 24.4 percent were between 25-29 years and 26.8 percent were 30 or above 30 years. The mothers who were participated in the study were mostly housewife while only 2.4 percent mothers were service holders. The mothers who were participated in the study, among them 40.2 percent did not have any literacy while 48.8 percent mothers completed their primary education. Very few percent of mothers completed secondary education (4.7 percent) and higher secondary education or above (6.3 percent). The mothers who were participated in the study, among them 63.8 percent were within normal BMI while 26.0 percent were under weight. While 10.2 percent were overweight. Findings from the study conducted by Azizur Rahman (2009) also suggest the similar findings. It was observed that the prevalence of severe and moderate wasting were more common among children, and the overall prevalence of acute malnutrition was about 10%, indicating that it is one of the major public health problems in the country. Multivariate analysis showed that mother’s BMI and media exposure, child’s age and birth size, and respiratory sickness in childhood were significantly associated with both severe and moderate wasting (Rahman,2009).
All the children weighted. Findings show that a significant percentage of children were less than 10 kg (81.1 percent) while 18.9 percent were above 10 kg. Findings show that 29.9 percent of children were less than 70 cm, while 63 percent were between 70-80cm and only 7.1 above 80 cm. The weight was measured according to age. Findings show that 14.2 percent of children were severely underweight, while 23.6 percent were moderately underweight. Findings show that among all children, 14.2 percent of children were severely stunting, while 29.9 percent were moderately stunting. According to the nutritional condition of the children was assessed by weight for height, 3.9 percent of children were severely wasting, while 11.0 percent were moderately wasting and 85 percent were within normal range. This findings differ from the national figure which much higher than this figure. This variation might be due to age limitation of the children (Rayhan et al. 2006). This study included children below 2 years while most of the national study showed the situation of children below 5 years age.
Study findings show that among 68 male children, 29 male children (42.6 percent) were underweight while among 59 female children, 19 female children (32.2 percent) were underweight. Similarly 48.5 percent male children were stunting and 39 percent female children were the same. In addition, 16.2 percent male children were wasting while it was 13.6 percent for the female children. This figure differs from the findings of the report of UNICEF. It might be due to selection of small number of sample and in selected villages.
Findings show that among 127 children, 23.7 percent children who were within age 6 month to 11 months were underweight while it was 42.1 percent for the age group 12 months to 17 months. Similarly, 45.1 percent children age 18 months to 23 months were underweight. The tendency of underweight increased with age. In case of stunting, 31.6 percent children who were within age 6 month to 11 months were stunting while it was 36.8 percent for the age group 12 months to 17 months. Similarly, 58.8 percent children age 18 months to 23 months were stunting. The similar relationship was observed regarding underweight and stunting and the age. For the case of wasting a different situation was observed. Twenty one percent children who were within age 6 month to 11 months were suffering from wasting while it was 7.9 percent for the age group 12 months to 17 months. Similarly, 15.7 percent children age 18 months to 23 months were suffering from wasting. Similar findings also revealed from other studies like Bairagi (1987) Black (1984) and Rahman (2009).
Findings show that the children who suffered from fever among them, 70.6 percent were underweight, 70.6 percent were stunting and 17.6 percent were wasting. Similarly, children who suffered from common cold and other respiratory diseases among them, 50 percent were underweight, 45.8 percent were stunting and 25 percent were wasting. It was also observed that children who suffered from diarrhea among them, 28.6 percent were underweight, 25 percent were stunting and 14.3 percent were wasting. It is important to note that the children who suffered from fever during the last 15 days of survey period were more likely to develop malnutrition followed by respiratory diseases and diarrhea. Similar findings also revealed from other studies like Bairagi (1987); Black (1984); Mozumder (2000); Dewan (2000) and Rahman (2009).
Findings show that there were only 14 mothers who were below 20 years of age. It was observed that 28.6 percent of the total children of the mother of age below 20 years were underweight while 57.1 percent were stunting and 7.1 percent were wasting. Among 127 children, 33.3 percent children whom mothers were aged between 20-24 years were underweight while it was 32.3 for stunting and 14.6 were wasting. Similar findings also were observed among the children whom mothers were aged between 25-30 years except for the cases of wasting which was higher among the children of mothers aged 25-30 years. Important findings observed among the children whom mothers were above 30 years of age. Fifty percent of the children were underweight; 58.8 percent children were stunting and 29.4 percent children were wasting whom mothers were above 30 years of age. It might be due to better awareness among the young mothers than that of older mothers.
Findings show that there were significant differences among the children by their nutritional status according their mother’s education. It was observed that higher number of children suffered from malnutrition whom mothers were illiterate. Forty percent children suffered from underweight; 66.7 percent suffered from stunting and 17.6 percent suffered from wasting among the total children and their mothers were illiterate. Similarly, 35.5 percent children suffered from underweight; 33.9 percent suffered from stunting and 12.9 percent children suffered from wasting among the total children and their mothers had primary education. Nutritional level was better among the children of mothers with secondary education. The nutritional status of under five children is a sensitive indicator of a country’s health status as well as economic condition. This study investigated differential impact of some demographic, socioeconomic, environmental and health related factors on nutritional status among under five children in Bangladesh. The analyses revealed that 45 percent of the children under age five were suffering from chronic malnutrition, 10.5 percent were acutely malnourished and 48 percent had under-weight problem. The main contributing factors for under five malnutrition were found to be previous birth interval, size at birth, mother’s body mass index at birth and parent’s education (Rayhan et al. 2006). Findings show that there were significant differences among the children by their family income. It was observed that higher number of children suffered from malnutrition whom family income was lower. Forty nine percent children suffered from underweight; 52.3 percent were stunted and 16.9 percent were wasting among the total children and their family income was 5000 taka or below. Similarly, 40 percent children suffered from underweight; 42.0 percent suffered from stunting and 12.0 percent children suffered from wasting among the total children and their family income was between 5000-10000 taka per month. Improved situation was observed among the children whom family income was above 10000 taka per month. Roy (2007) also revealed that there are strong relation between mother’s education and other socio-economic condition and nutritional status of children.
LIMITATIONS
The study was conducted with very few numbers of participants in four selective villages. In addition, the study was conducted in such villages where BRAC has been working for a long time. So there is a contamination of result from other study due to intervention of BRAC, although there was no nutrition program. In addition, due to time shortage and financial constraint, the study was conducted for a short time and most of the history was taken from the mothers. It would be better if the study could observe the caring practices of mothers in the study area.
CONCLUSION AND RECOMMENDATIONS
Improving nutrition can have a significant impact on survival as well as physical and cognitive development of the children. Good nutrition, comprising adequate quality and quantity of food intake and reduction of illness is also a basic human right and is an essential input for economic development. Hygiene awareness is essential to improve the caring practices of mothers to prevent malnutrition among the children under 5 years of age.
Recently the government of Bangladesh and interested organizations has started to increase the awareness level on reduction of malnutrition among children as well as the women. Greater attention is being given to supportive policies for continuous support the rural community and also increase the number of research study to identify the barriers of improving nutritional level of the children.
The study findings recommend the followings:
- A wide range of study should be conducted in Bangladesh for generalize the findings.
- Continuous awareness rising activities should be delivered at grass root level.
- Research should be a part of any intervention to see the impact, barriers to achieve goals, and opportunities to improve the nutritional level of children.