Preface
Social work education seeks to provide information, knowledge and skills to people who wish to work in the field of social work. Field work is an integral part of the total social education. Historically the profession of social work has considered field work a primary means of providing students the opportunity to integrate knowledge, value and skill.
Field work brings this golden opportunity to an apprentice social worker to use his /her knowledge on social work effectively in execution, to acquire certain skills which are raley learnt in the classroom and thus to bridge the divide between the classroom and the real world .For this reason field work has been included in the syllabus of social work education and I was sent to an agency named BIRDEM Hospital , Dhaka.
This report has been prepared on the activities I have done during 60 working days of my fieldwork. My first duty was to know about the agency and the agency which I have descried in the second and third chapter. Before this in the first chapter, I have given some definition and important of field work in brief. Another important duty bestowed on me was to study some cases as part the application of social work methods. Information I have collected by studying the cases have been in the fifth chapter. Fourth chapter includes performed duty and responsibilities.
In essence, this report is a presentation of what I have seen and what I have done in the course of field work.
Preamble
Social work is a helping profession which fundamentally and radically aims to assist the individuals,groups and community to cope with their complex socio-economic psychological problams enabling them.so that they can solve their problam by helping themselves.according to one of the great pioneer walter a friedlander,social work methods are divided into two part (a)Basic methods of social case work (b)Auxiliary .Basic method are divided into three parts such as (1)Social case work (2)Social group work (3)community social work .Auxiliary methods are divided into three parts such as (1)social action (2)social administration (3)social research .
Social work in practice is called field work. It relates particularly in care , particularly in group and particularly a student cannot get practical knowledge about the field where he or she is going to work in near future . Therefore field work is a rare combination of theoretical and practical knowledge and it makes a bridge among the people to solve the psycho-social and other complex problem . In this field new scholar become skilled interviewing , using theories , methods ,thecniques in practical arena assuring recording , responding reporting etc .After all social worker diverts problem from complexity to simplicity
INTRODUCTION
“Social Work is the dual focus on person and environment , with the emphasis placed on interactions and transactions between them, that sets social work apart from other helping disciplines”1. Social work in its various forms addresses the multiple, complex transactions between people and their environments. Its mission is to enable all people to develop their full potential, enrich their lives, and prevent dysfunction. Professional social work is focused on problem solving and change. As such, social workers are change agents in society and in the lives of the individuals, families and communities they serve. Social work is an interrelated system of values, theory and practice. Field work is the way of getting social work students used to with the diverse fields of social work interventions. Field work may to build a bridge between community and academic education. It can be viewed the following Figure:
SOCIAL WORK
Social work developed as a 20th century profession out of its voluntary philanthropy and social reform roots. These roots are deeply linked to ancient values and concepts of charity, equality and compassion toward others in times of need. The profession’s contemporary roots are particularly connected to social welfare developments in the 19th century.
These developments included reform movements to change negative societal attitudes toward people in need; charity organization societies to help individuals and families; settlement houses to improve living conditions at the neighborhood level; and rising feminist advocacy for human rights, social justice and gender equality.
The profession of social work is uniquely founded on altruistic values respecting the inherent dignity of every individual and the obligation of societal systems to provide equitable structural resources for all their members.
Social work’s primary concern is the social well-being of all people equally valued with the importance of their physical, mental and spiritual well-being. Social work pioneers were among the first to address the significance of deeply connected relationships that constitute the social context of people’s lives. Out
of this rich heritage social work is recognized for its familiar “person-in-environment” perspective, which characterizes the unique relationship-centered focus of the profession. Parallel advances in other fields now provide significant support for the on-going advancement of social work as a relationship-centered profession with a repertoire of person- and environment-oriented methods of practice.
International federation of social worker has defined social work as such: The social work profession promotes social change, problem solving in human relationships and the empowerment and liberation of people to enhance well-being. Utilizing theories of human behavior and social systems, social work intervenes at the points where people interact with their environments. Principles of human rights and social justice are fundamental to social work.
According to National Association of Social Worker “Social Work is the professional activity of helping individuals, groups, or communities enhance or restore their capacity for social functioning and creating societal conditions favorable to this goal. Social Work practice consists of the professional application of Social Work values, principles, and techniques to one or more of the following ends: helping people obtain tangible services; counseling and psychotherapy with individuals, families, and groups; helping communities or groups provide or improve processes. The practice of Social Work requires knowledge of human development and behavior; of social, economic, and cultural institutions; and of the interactions of all these factors. Social Work is concerned and involved with the interactions between people and the institutions of society that affect the ability of people to accomplish life tasks, realize aspirations and values, and alleviate distress. These interactions between people and social institutions occur within the context of the larger societal good. Therefore, three major purposes of social work
may be defined
►to enhance the problem-solving, coping and developmental capacities of people;
►to promote the effective and humane operation of the systems that provide people with resources and services;
►to link people with systems that provide them with resources, services, and opportunities.
SOCIAL WORK VALUES
Social work grew out of humanitarian and democratic ideals, and its values are based on respect for the equality, worth, and dignity of all people. Since its beginnings over a century ago, social work practice has focused on meeting human needs and developing human potential. Human rights and social justice serve as the motivation and justification for social work action. In solidarity with those who are dis-advantaged, the profession strives to alleviate poverty and to liberate vulnerable and oppressed people in order to promote social inclusion. Social work values are embodied in the profession’s national and international codes of ethics.
SOCIAL WORK THEORY
Social work bases its methodology on a systematic body of evidence-based knowledge derived from research and practice evaluation, including local and indigenous knowledge specific to its context. It recognises the complexity of interactions between human beings and their environment, and the capacity of people both to be affected by and to alter the multiple influences upon them including bio-psychosocial factors. The social work profession draws on theories of human development and behavior and social systems to analyze complex situations and to facilitate individual, organizational, social and cultural changes.
SOCIAL WORK PRACTICE
Social work addresses the barriers, inequities and injustices that exist in society. It responds to crises and emergencies as well as to everyday personal and social problems. Social work utilizes a variety of skills, techniques, and activities consistent with its holistic focus on persons and their environments. Social work interventions range from primarily person-focused psychosocial processes to involvement in social policy, planning and development.
These include counseling, clinical social work, group work, social pedagogical work, and family treatment and therapy as well as efforts to help people obtain services and resources in the community. Interventions also include agency administration, community organization and engaging in social and political action to impact social policy and economic development. The holistic focus of social work is universal, but the priorities of social work practice will vary from country to country and from time to time depending on cultural, historical, and socio-economic conditions
Development of field work
On the view of field work social work is a dynamic and updated discipline than the other discipline of arts and social science faculty. But field work is not a ready made product of present time. It show an aged history like social work education initial stages of field work was not systematic and organised. One of the great pioneers of the social work mary richmond first introduced social work practice and she wrote a dramatic and historical book named ‘social Diagonosis’ which worth,P.I. Park and has inaugurated the medicalfield practice at the chicago university of america to evaluate and monitor urban poverty by their student . Dr. Emerson has taken initiative to send the medical student to social agency at the john Hopkins University in 1920.
Fieldwork practice is indispensible part of social work education .National social service Academy of social service Department of the Peoples Republic of Bangladesh has organized short training course for its Social Services officers and field worker in 1963 .Generally three type training has organized by the department like internal training ,primary training and refers course.
From the mid 18th century to the end of the 19th century social work has evolved from societies to assist and reform a year of full time academic study .Now all over the world there are many course on social work education .After the indepence from british , india,pakistan was facing many socioeconomic problems and government sought United Nations help.After government request UN sent an expert team .According to their recommendation a short course of three months were introduced in 1953 to produce social worker .
In the meaning V-AID programe in 1953 and urban community development program were expanding quickly by government and voluntary organization .As a result concerned authority felt the need of starting higher education on social work.And in 1959 Dhaka University started MA course on social work and also established social work college and research center which was inaugurated by Lt Colonel Azam khan on 19th March 1963 for its own building .In 1958-59 social welfare college and research , in 1965 Rajshahi University and in 1992-93 Shahjalal University and under national University started compulsory field work .Hon’s and Masters Degree .
GOALS AND OBJECTIVES OF FIELD WORK PRACTICE
Field work provides students with genuine experiences in applying social work methods and it enables them to become familiar with the real work practice. the major objectives of the field work is to provide planned observations and practical demonstration in the selected fields of social work which are being analyzed in the classes.
R.R Sing (1985, 44-45) in Field work in social work education has mentioned the following objectives:
- To offer purposeful learning experience to students through interaction with life situations under supervisory guidance for professional growth in terms of knowledge, skills, and attitudes.
- To foster attitudes in the student towards professional self development, increasing self awareness appreciation of both capacities and limitations.
- To develop in the student the required skills in helping the needy through organizational work, use of social work methods, that is, listening, participating communication and so on. And
- To enable the student to develop and deepen capacity to relate theory to practice and also to relate experience to theory.
The view committee on social work education in India has mentioned the following objectives:
- Development of skills in problem solving at the mean and macro mentioned
- Integration of classroom learning with field practices
- Development of skills for professionals practice at the particular level of learning
- Development of professional attitudes , values and commitments
- Development of self awareness and professional ideas.
Font of the above decision, we can summarize as below:
- To acquire the real knowledge by applying all theoretical knowledge.
- To help students learn how to think critically, analytically and evaluative, so that their talent can be developed.
- To help students develop the capacity to establish and maintain professional relationships
- To help students develop a high degree of social awareness and a deeper understanding the democratic process.
- To help students develop their professional selves, including some ability to evaluate their own capacities to help people. This is seen as including identification with profession and is understood in terms of progress the students make in identifying with the school and with his field work agency.
- To help students master a substantial body of conceptual knowledge regarding individual, group and societal behavior.
- To develop of skill in helping, involving the disciplined use of knowledge in thinking about analyzing and understanding professional problems and in the helping process.
- It tries to develop professionalism and professional discipline among social worker.
Definition
The term diabetes mellitus describes a metabolic disorder of multiple aetiology characterized by chronic hyperglycaemia with disturbances of carbohydrate, fat and protein metabolism resulting from defects in insulin secretion, insulin action, or both. The effects of diabetes mellitus include long–term damage, dysfunction and failure of various organs. Diabetes mellitus may present with characteristic symptoms such as thirst, polyuria, blurring of vision, and weight loss. In
its most severe forms, ketoacidosis or a non–ketotic hyperosmolar state may develop and lead to stupor, coma and, in absence of effective treatment, death. Often symptoms are not severe, or may be absent, and consequently hyperglycaemia sufficient to cause pathological and functional changes may be present for a long time before thediagnosis is made. The long–term effects of diabetes mellitus include progressive development of the specific complications of retinopathy with potential blindness, nephropathy that may lead to renal failure, and/or neuropathy
with risk of foot ulcers, amputation, Charcot joints, and features of autonomic dysfunction, including sexual dysfunction. People with diabetes are at increased risk of cardiovascular, peripheral vascular and cerebrovascular disease. Several pathogenetic processes are involved in the development of diabetes. These include processes which destroy the beta cells of the pancreas with consequent insulin deficiency, and others that result in resistance to insulin action. The abnormalities of carbohydrate, fat and protein metabolism are due to deficient action of insulin on target tissues resulting from insensitivity or lack of insulin.(WHO,1999)
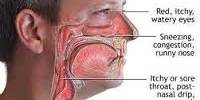
Symptoms
High blood levels of glucose can cause several problems, including:
- Blurry vision.
- Excessive thirst.
- Fatigue.
- Frequent urination.
- Hunger.
- Weight loss.
TYPES OF DIABETIS
Type 1 diabetes mellitus
Type 1 diabetes mellitus is characterized by loss of the insulin-producing beta cells of the islets of Langerhans in the pancreas leading to insulin deficiency. This type of diabetes can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, where beta cell loss is a T-cell mediated autoimmune attack.[6] There is no known preventive measure against type 1 diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults but was traditionally termed “juvenile diabetes” because it represents a majority of the diabetes cases in children.
Type 2 diabetes mellitus
Type 2 diabetes mellitus is characterized by insulin resistance which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor. However, the specific defects are not known. Diabetes mellitus due to a known defect are classified separately. Type 2 diabetes is the most common type.In the early stage of type 2 diabetes, the predominant abnormality is reduced insulin sensitivity. At this stage hyperglycemia can be reversed by a variety of measures and medications that improve insulin sensitivity or reduce glucose production by the liver.
Gestational diabetes mellitus
Gestational diabetes mellitus (GDM) resembles type 2 diabetes in several respects, involving a combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2%–5% of all pregnancies and may improve or disappear after delivery. Gestational diabetes is fully treatable but requires careful medical supervision throughout the pregnancy. About 20%–50% of affected women develop type 2 diabetes later in life.
Even though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother. Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit fetal surfactant production and cause respiratory distress syndrome. Hyper bilirubinemia may result from red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor placental perfusion due to vascular impairment. Labor induction may be indicated with decreased placental function. A cesarean section may be performed if there is marked fetal distress or an increased risk of injury associated with macrosomia, such as shoulder dystocia.(WHO,1999)
Two very important concepts are related to the diabetes patients. These are,
- Hypoglycemia and ,
- Hyperglycemia.
Hypoglycemia
Levels which are significantly above or below this range are problematic and can in some cases be dangerous. A level of <3.8 mmol/L (<70 mg/dL) is usually described as a hypoglycemic attack (low blood sugar). Most diabetics know when they’re going to “go hypo” and usually are able to eat some food or drink something sweet to raise levels. A patient who is hyperglycemic (high glucose) can also become temporarily hypoglycemic, under certain conditions.
Hyperglycemia
Hyperglycemia, or high blood sugar, is a condition in which an excessive amount of glucose circulates in the blood plasma. This is generally a glucose level higher than 10 mmol/l (180 mg/dl), but symptoms may not start to become noticeable until even higher values such as 15-20 mmol/l (270-360 mg/dl). However, chronic levels exceeding 7 mmol/l (125 mg/dl) can produce organ damage.(online, accessed on, o8.03.2011)
Treatment of diabetes
Diabetes is a life time disease. It can’t be removed; only following some criteria a diabetes patient can control his disease.
For controlling the disease four rules need to follow.
- Diet control.
- Physical exercise or discipline.
- Drug.
- Education.
First 3 steps are generally known as 3D. These are the main treatment for a diabetes patient for his/her happy and natural life.
DIABETIC ASSOCIATION OF BANGLADESH ( BADAS)
The comprehensive health care delivery to a vast number of diabetic all over the country is well recognized as a unique program of the Diabetic Association of Bangladesh (BADAS). The Association executes this program primarily through its central institute called the Bangladesh Institute of Research &Rehabilitation in Diabetes, Endocrine and Metabolic Disorders (BIRDEM).
BIRDEM as a sister concern of BADAS going the right way to fulfill the goals and objectives of the association for diabetic patient. But before going to the introduction of BIRDEM, here in some words that will describe the diabetic association of Bangladesh.
The Diabetic Association ofBangladesh was established on 28 February 1956 in Dhaka at the initiative of the late National Professor M Ibrahim and a group of social workers, philanthropists, physicians and civil servants. The Association started an out-patient clinic in 1957 in a small semi-permanent structure of about 380 sqft at SegunBagicha, Dhaka. Over the years, the clinic has turned into a diabetes care and research complex at Shahbag, Dhaka, which, after the demise of Prof M. Ibrahim in 1989, has been renamed as the Ibrahim Memorial Diabetes Centre.
BADAS is a nonprofit voluntary socio-medical service organization registered with the Ministry of Social Welfare under the Society‘s Registration Act, 1860. It is run by a 32 member National Council of which 18 members from the life member category and 6 members from the affiliated association category are directly elected. One-third of the members from the life member category and 2 from the affiliated association retire every year by rotation and election to those one-third posts is held in every Annual General Meeting of the Association. The elected members elect the office-bearers of the National Council, consisting of a President, 3 Vice-Presidents, a Secretary General, a Join Secretary General, a Treasurer and a Joint Treasurer.
The President, so elected, nominates another 5 members from amongst the Vice-chancellors, Professor of Universities in Bangladesh, Heads of NationalResearch Organizations, Heads of Financial institutions, Heads of Donor Agencies, Heads of Social Welfare Organizations, Heads of Professional bodies and reputed social workers. In addition, the Government nominates 3 ex-officio members representing the Ministries of Health and Family Welfare, Social Welfare and Finance. The members nominated by the Government must be in the rank of or above of a Joint Secretary.
The National Council meets at least once a month and reviews the activities of the Association. It takes decisions on policy, budget and finance, planning and development. The executive power of the National Council is vested with the Secretary General who runs the different institutions throng respective Board of Management with the help of the Treasurer, BADAS Secretariat and BADAS Project Office. (BIRDEM annual report, 09)
Dr. Ibrahim and the DIABETIC ASSOCIATION OF BANGLADESH
Dr. Ibrahim, the founder of DIABETIC ASSOCIATION OF BANGLADESH who was the precedent of the BADAS till his death born in kharrera village, near murshidabad of India in 31st December in 1911. From the childhood he was shows his sign in study by performing meritorious performances. In 1938, after passing from Calcutta medical college with MB degree, he started his carrier.
From 1938 to 1945 he worked as a house physician, emergency medical officer and senior demonstrator of pharmacy department in Calcutta medical college. In 1945 he starting working as a resident physician, and worked there till 1947. After 1947 he came to the east Pakistan and joined as a civil Carson of Chittagong. In the same time he was appointed as a superintendent of Chittagong medical college and hospital. He was a teacher of medicine in the same time.
In 1948 he went to England for attending the M.R.C.P degree, and came out successful in the next year. He went American college of chest physician of U.S.A in 1949 for attending F.C.C.P. degree. After returning home in 1950 he was appointed as a additional physician of Dhaka medical college. After some time he became professor of clinical medicine.
During his time in the Dhaka medical college, he formed Pakistan diabetic association. And the date was 28th February of 1958. The day of 28th February is celebrated as diabetic awareness day in Bangladesh. He was governor of Pakistan chapter of American college of chest physicians. In 1962 he got F.C.P.S. degree from the Pakistan college of physicians. During 1962-1964 he worked as a professor of medicine and principle of sir salimullah medical college. He was selected to have SITARA E KHIDMAT from the government of Pakistan for contributing to medical profession of Pakistan.
In 1964 he was appointed as a professor and director of Jinnah post graduate medical center. In that time he was working for the welfare of the diabetic patient, and formed diabetic association of Pakistan in Lahore and Karachi. In 1967 he got the magical degree of F.R.C.P. from the royal college of physicians. His contribution to the science and technology was to high, that the government chose himself as the president of national science council. He worked in there for two years in the time period of 1969-70.
After the liberation war dr.Ibrahim came back to his motherland, and started working to the medical branch, as well as in the social services. No doubt his working ground was mainly centered by the diabetic patients. From 1972-82, he was the president of bangladesh association of scientists and scientific proffesions.In 1978 he went for F.R.C.P. from the royal college for physicians.
Not only he was a doctor, but contributes to the national development by working along with the political movements. He joined the ministry of labor and manpower in 1975. In the same time he was the advisor of president of the democratic republic of Bangladesh. He was also the president of BangladeshCollege of physicians.
He was announced for the independent day prize in 1979 which is the most honorable prize and most respectful award of Bangladeshi people. He worked as the president of Bangladesh science council from 1981-82. In 1981 he was elected senate member of university of Dhaka.
He worked as a member of managing committee of international diabetic federation.
In 1984 he again announced for independent day prize, in this time it was for diabetic research, treatment, and for BIRDEM. In the same year he was announced the national professor. And this is to remember that he was the first doctor to achieve this title.
In the next year he was announced the fellow of Bangla academy, and in 1986 he was announced fellow of international islami academy of science.
It was 12:30 pm of 6th September of 1989 when this great doctor and social worker, died after just returning from abroad to his home.(shoronika,2006 )
Here is few steps which will describe the history of Bangladesh diabetic association.
- The first meeting of the diabetic association was held on the 28th February of 1956, and the place of that meeting was, the resident of the dr. md. Ibrahim.
- Establishment of the medical research center in 1957
- In 1959 the diabetic association got the membership of the “INTERNATIONAL DIABETIC FEDARATION”.
- During the month of march of 1967 diabetic hospital opened its emergency unit.
- The month of January in 1968 the first rehabilitation center opened.
- April of 1968, the applied nutrition training and research institute established.
- In 1975 the association got assistance from WHO.
- In 1977 birdem started building its own structure at shahbah in Dhaka.
- For the first time the WHO organize a post-graduation course titled “diabetic endocrine and metabolic disorder”.
- The national council in its 178th meeting took decision to create a fund for the diabetic federation.
- Bangladesh diabetic association got elected in the presidential council of international diabetic association.
- At last in 1980 BIRDEM got established.
The activities of DIABETIC ASSOCIATION OF BANGLADESH
DIABETIC ASSOCIATION OF BANGLADESH has some major activities for reaching its goals and objectives. This programs are creating the awareness among the people and the diabetes patient as well as creating a strong structure for preventing the disease.
The activity follows in brief.
Training program: DIABETIC ASSOCIATION OF BANGLADESH is running training programs with the association of WHO for the doctors, nurses, paramedics, social workers to let themselves know about the diabetes disease.
Research program: one of the biggest programs of DIABETIC ASSOCIATION OF BANGLADESH is to conduct research program about the causes, treatment method, side effect of the treatment and relater many other topic with diabetes.
Publications: DIABETIC ASSOCIATION OF BANGLADESH always try to speak out about this disease, and organize seminars, symposiums, and publishes booklets, journals, and tv programs.
Training and research: for ensuring the nutrition for the poor patient, theDIABETIC ASSOCIATION OF BANGLADESH established a center in jurain, Dhaka. It ensures the nutrition and research as well as the education program for patients.
Treatment facilities: DIABETIC ASSOCIATION OF BANGLADESHensure the best use of its resources by giving the poor patient free treatment and drugs with the help of social welfare department who follows the skill and principle of social work profession.
Motivation program: DIABETIC ASSOCIATION OF BANGLADESH continuously organize discussion meetings, treatment camps, and motivation program such as visiting home of patients, motivating the family member.
Hospital facilities: DIABETIC ASSOCIATION OF BANGLADESH has a large 600 bedded modern diabetes hospital called BIRDEM in shahbag. It also has branches of it all around the country.
Rehabilitation program: The association trains the poor patients in income earning activity and rehabilitates the patients in their respected family and society.
Right now BIRDEM has following departments.
- Clinical Services Division.
- Out-Patient Department.
- Department of Diet and Nutrition.
- Department of Dentistry.
- Department of Dermatology.
- Department of Physical Medicine &Rehabilitation.
- Department of Social Welfare.
- Department of Public Relations.
- In-Patient Service Departments.
- Department of Internal Medicine, Oncology, Rheumatology& Hematology (I& II).
- Department of Gastrointestinal, Hepatobiliaryand Pancreatic Disorders (GHPD) MU-II.
- Department of Nephrology (Unit-I).
- Department of Endocrinology and Pulmonology.
- Department of Internal Medicine and Neurology (I&II).
- Department of Critical Care Medicine.
- Department of Cardiology.
- Department of Pediatrics and Neonatology.
- Department of Gynecology and Obstetrics.
- Department of Surgery.
- Department of Urology.
- Department of Ear, Nose & Throat Disease and Head & Neck Surgery.
- Department of Orthopedics and Traumatology.
- Emergency Unit.
- Finance and Accounts Division.
- Department of Nursing.
- Library.
- Department of Radiology & Imaging.
- Dept. of Biochemistry and Cell Biology.
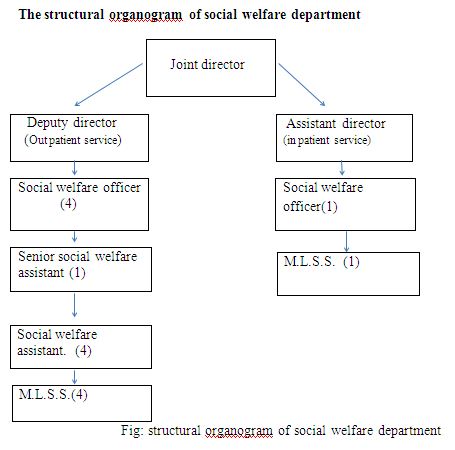
Department of Social Welfare
The Department of Social Welfare started its service from the beginning of the birth of BIRDEM. The duty of this department is to collect the socio-economic, personal and medical records of the needy patients who do not belong to run their treatment without any help of the external support. This department also fixes the amount of help a patient is going to get for rest of his life. The Social Welfare Department has always been rendering services to the diabetic patients to uphold and improve their life-level, especially to help them to lead a normal self-dependent and useful socio-economic life. Again to improvise and standardize their compliance of health care, educational emotional support, motivation and follow-up activities of this dept. are being carried out regularly.
Further, in order to facilitate care and treatment of poor, under privileged patients having outside Dhaka are being referred and insulin injections are sent to their nearest Branch. Association and Thana Health Complexes. During the period under review the diversified services rendered in terms of need of the patients, are as follows.
- Attended Patients with medico-social, socioeconomic and psycho-social problems.
- Patients with emergency medical need, compli-eations ant special problems are helped to get needed care and treatment.
- Social study done for social diagnosis and recorded useful information.
- Patients who have discontinued treatment were helped to get treatment and motivated to follow diabetes regimen.
- Educational, motivational and follow-up services rendered to patients
- Training and retraining on methods and techniques of insulin administration imparted
- Helped to get in-patient services from other medical institutes.
- Home visits for social diagnosis.
- Social rehabilitation
- Young unemployed and under employee diabetics are rehabilitated in gainful employment.
- Assessment of patients.
- Insulin injections supplied to the poor patients of OPD on concession and free of cost
- Insulin supply to non-paying ward,
- Insulin supply to poor patients of remote places by post through Thana Health complexes.
- Insulin supply to poor patients free of cost and on concession through Branch association.
Duties and Responsibilities bestowed on me
During my field work in BIRDEM I had some duties on me from my institute supervisor and my agency supervisor. The kind of duties I tried to completed, those are;
Duties from the institute supervisor
- To go to the agency in time and obey the agency supervisor.
- Keep the daily record in the process recording book.
- Listen and attend the supervisory conference.
- Take at least 4 cases for the finale field work report.
- Prepare a finale field work report.
- Use the social work and skills effectively in the knowledge problem solving process.
Duties on me from the agency super visor
- Sign the attendance register regularly.
- Create a good relation among the working stuff, and make rapport with the client.
- Learn about the different unit and department of agency.
- Learn the structure, objectives, goals and programs of the agency.
- Help the client to have their service, by taking their interview.
- Collect data about the social, economic condition.
- Take the case history effectively.
- Make follow up with full attention to the client.
- Visiting the home of selective clien
Mainly I have conducted 4 kind of job. These are;- Case history.
- Follow-up.
- Home visit.
- Working with the problematic patients.
List of home visit which I completed
Home visit :01
Name of client :Forhad Hossain
Reference number:246537
Social welfare number:459605
Address:Pilkhana road,lalbagh
Age:50
Date:29 /08/2012
Information about home:Forhad hossain lives on the 3rd floor of a six stories building with his family member.The building is very much vulnerable to live.
Information about furniture:Mr. Forhad have two bed,a study table , a colourful television , a daining table, a rack , a weardrobe etc.
Family structure:Mr. forhad family consist of five member.He has two sons and a daughter.His elder son completed higher secondary (H.S.C) .And younger son is a higher secondary student. Both of his son tries to help father through involve in tution.Only daughter chadney is a class seven student of agrani school.Forhad wife sell handmade bags.
Socio-economic condition:Client socio-economic condition is very poor.
Monthly income-
income of elder son-4000tk
income of younger son-4000tk
income of wife -6000 tk
Monthly expenditure-
house rent-6000 tk
household cost-6000tk
cost of daughter education-400 tk
cost of client medicine-1500 tk
Opinion of neighboure :Afruit seller beside forhad hossain house said that Mr.forhad and his family leads a nominal life.
My opinion :All information that he gave is true .He lives in a vulnerable condition.He should continue get help from BIRDEM.
Case No :02
Name of client :Soma begum
Reference number:413647
Social welfare number:587349
Address:Dilu road road,mogbazar
Age:45
Date:26 /09/2012
At 9:00am i came out from my home to do a home visit.Name of my client is soma begum; lives in dilu road mogbazar.At 9:30 am i along with my field work friend maksuda akter ride a bus from nilkhat to mogbazar.At 11:30am we can find out the house of soma begum.Description of home visit on soma begum given below:
Information about home:Client soma begum lives ground floor of a four stores building in dilu road,mogbazar. She lives in a single room with her family.The building is very much vulnerable to live.
Information about furniture:The client have a bed, a colourful television , a frezz, a rack , a weardrobe a showcase etc.
Family structure:At present the number of family number of.family member is 03. she has a son and two daughter.har only son lives in mirpur with his family and he is a driver.her younger daughter got married.her elder daughter lives with them and she is garments worker.her husband is a salesmen of a roadside tea-stall
Socio-economic condition:Client socio-economic condition is very poor.
Monthly income-
Huband income -4000tk
client income -1500tk
Daughter income -4000 tk but give 2000tk
Monthly expenditure-
house rent-4000 tk
household cost -6000 tk
cost of client medicine-1000 tk
Opinion of neighboure :Neighbour of soma begum said that the economic condition of soma begum is not good.
My opinion :All information that she gave is true. Her son stay away and never gave finicial support to them.She need free service from BIRDEM
Case No :03
Name of client :Roksana akhter
Reference number:463784
Social welfare number527539:
Address : 375/A Modubagh,mogbazar
Age:46
Date:27 /09/2012
At 9:00am i came out from my home to do a home visit.Name of my client is soma begum; lives in dilu road mogbazar.At 9:30 am i along with my field work friend maksuda akter ride a bus from nilkhat to mogbazar.At 11:30am we can find out the house of soma begum.Description of home visit on soma begum given below:
Information about home:Client Roksana lives 1st floor of a two stores building in modubagh ,mogbazar. She lives in a single room with her family.
Information about furniture:The client have a bed, a colourful television , a rack , some plate and cooking materials etc.
Family structure:At present the number of family number of.family member is 03. she has a son and two daughter.har only son lives in mirpur with his family and he is a driver.her younger daughter got married.her elder daughter lives with them and she is garments worker.her husband is a salesmen of a roadside tea-stall
Socio-economic condition:Client socio-economic condition is very vulnerable.
Monthly income-
Huband income -6000tk
client income -1500tk
Sonsr income -3000 tk
Monthly expenditure-
house rent-3300 tk
household cost-5000tk
cost of client medicine-1500 tk
cost of daughter education -500 tk
Opinion of neighboure :Neighbour of Roksana said that the economic condition of roksana begum is not good.
My opinion :All information that she gave is true.Her economic condition is vulnerable.She need free service from BIRDEM .
Home visit No :04
Name of client :Joya Gosh
Reference number :465378
Social welfare number:59237
Address : 61/2 Goalnagor,english road
Age:50
Date: 27 /10/2012
At 9:00am i came out from my home to do a home visit.Name of my client is joya gosh; lives in goalnagor,english road.At 9:30 am i along with my field work friend assudazaman ride a ricksha from nilkhat to english road.At 11:30am we can find out the house of Joya Gosh.Description of home visit on soma begum given below:
Information about home:Client Joya gosh lives with her sister family at 1st floor of a two stores building. She sleep on the floor.
Information about furniture:The client have no mentionable furniture at all.There is no bed.They have a rack and some cooking materials.
Family structure:joya gosh have two daughter.her elder daughter got married.and her younger daughter is missing
Socio-economic condition:Client socio-economic condition is very vulnerable .JOY gosh earn taka 30-40 per day by selling water.
Opinion of neighboure :according to the opinion of a female eighbour of her sister house joya gosh leads a vulnerable life.her sister husband behave with her rudely
My opinion :All information that she gave is true.Her economic condition is vulnerable.She need free service from BIRDEM .
Case study : 01
Personal information of the client
Name- Kamrun begum
Age-50
Sex-female.
Fathers name- Md.abul kalam
Mothers name- shamsun nahar.
Marital status- married.
Husbands name- Md sakander ali molla
Institutional identification number
Registration number- 459307
Social welfare number-59704
The amount of assistance the patient get from the agency
Insulin- 50% free
Investigation- 25% free
Drugs and hospital service-100% free.
Treatment information
Word no-92
Bed no- 926
Treatment method- conservative treatment.
Date of admission- 03/09/12
Date of release-17/10/12
Family structure
| name | Relation with the patient | Age |
| MD. sakander ali molla | husband | 60 |
| Fayej uddin | Son | 36 |
| moksud | Son | 30 |
| Sima begum | Daughter -in-law | 28 |
Permanent address
Vill- jorapukaria.
Post- cinakhora.
Thana- sujanogor.
District- pabna.
Rationality of taking case
With the kind permission of our agency supervisor visited the word which in under control of social welfare department. In the word number 92, I found a aged women laying on her bed, and crying. No one was near to her. I went to her, and start talking. After some time I understand she is a problematic patient. I may have some scope of using my social work knowledge, and skill to solve her problem. After talking to the nurses I decide to take her as my problematic case.
Present physical condition.
The Present physical condition of my patient are-
- 2 month infection in right leg.
- Low weight.
- Skin diseases.
- Malnutrition.
Sources of collection of data
| Primary data | Secondary data |
| Talking to the patient. | Record of patient from social welfare department. |
| Talking to the medical stuff. | Medical record. |
Treatment.
She got conservative treatment during her days in the hospital. Doctors advised for two insulins.
Actrapid (40 u) 04+04+08
Insulatard(100 u) 08+00+06
Rapport building
During her stay in BIRDEMI used to visit him almost daily. I tried to explore the factors regarding her disorder and sometime I gave her mental support. Thus she began to take me as a well-wisher and there created a good relation between us.
Family condition.
The patient karimon begum is the 3rd child of her parents. She has two sons aged 38 and 30, and four daughter sister . All her daughter got married.her husband was a farmer but now he can not do any work beacuse of old age complication.Her two son works as a farmer in others field.
Social condition
My patient came from a middle class family, and her father is a respected man in his surroundings, just like my patient father in law. So social acceptance and cultural coping to the other family was not a big problem to my client.
Economic condition
Husband of karimon is now unemployed. His only source of income is her two sons monthly income.Her two son earn only tk 6000 per month . So it may say that my client is suffering from economic uncertainty.
Mental condition
From the very first day I meet kamrun she was very upset, and crying. After talking I understand she is having mental unrest, caused by her family condition, her economic uncertainty, and for her physical condition. in 2 month . The hospital stuffs were little worried about her mental unrest, she was not taking her insulin and drugs in time witch were making her shakier.
Problems I identified
- Lacking of knowledge about diabetes.
- Mental unrest.
- Economic uncertainty.
- Relationship problem with her husband.
- Lacking of knowledge about infection.
- Uncontrolled diabetes.
Problem solving process
For solving her problem, I followed two process which are important in social case work.
- Supportive treatment method.
- Correctives treatment method.
Supportive treatment method
Using this method I gave advice to her about how to control the diabetes, we had few open discussion about her family problem, I behave demonstratively to let she know that the kind of problem she is facing Is not unique, and many way is still open f solving those problems.
I also gave her relative information about the self-employment for her husband, and about the social welfare department who are providing her a handy service to her and for her betterment.
Correctional treatment method
In this phase, I let her know about the perfect lifestyle, the family function, and disciplinary life for controlling this disease, taking the insulin regularly, and coordinate her family and to her lifetime disease.
Evaluation
I left no stone unturned to help her. When she released from the hospital I gave her some advice that would be very much conducive for her. I wish her soon recovery.
Case history -02
Personal information of the client
Name- Tanvir ahmed.
Age-51
Sex-Male.
Fathers name- late saiyed ahmed
Mothers name- morzi begum.
Marital status- married.
Wife s’ name- dilara begum.
Institutional identification number
Registration number- 223089
Social wefare number-22580
The amount of assistance the patient get from the agency
Insulin- 80% free
Investigation- 80% free
Drugs and hospital service-100% free.
Treatment information
Word no-63
Date of admission- 12/12/10
Date of release-1/03/11
Bed no- 649
Treatment method- operative treatment.
Permanent address
Vill- debidar.
Post- debidar.
Thana- halishahar.
District- Chittagong
Family structure
| name | Relationship with client | Age |
| Delara begum | wife | 45 |
| sohrab | son | 24 |
| Rabbi | son | 20 |
| Chaiti | Daughter | 12 |
Rationality of taking case
With the kind permission of our agency supervisor visited the word which in under control of social welfare department. In the word number 63, I found a man of middle age laying on his bed, he has bandage in his left leg, and the picture wasn’t very attractive. His wife was near him. I went to him, and start talking. After some time I understand he is a problematic patient. I may have some scope of using my social work knowledge, and skill to solve her problem. After talking to the nurses I decide to take him as my problematic case.
Sources of collection of data
| Primary data | Secondary data |
| Talking to the patient. | Record of patient from social welfare department. |
| Talking to the medical stuff. | Medical record. |
Physical condition
The Present physical condition of my patient are-
- Cellulites and obsess of left foot.
- Uncontrolled diabetes.
- Low weight.
- Unemployment.
- Physical weakness.
- Worried about his future.
Treatment.
he got operative treatment during his days in the hospital. He was sent to operation theater twice, first on 23/12/10, and then on 10/102/11. Doctors advised for two insulin.
Actrapid (100 u) 10+8+6.
Insulatard (100 u) 0+0+6.
Rapport building
During his stay in BIRDEMI used to visit him almost daily. I tried to explore the factors regarding her disorder and sometime I gave her mental support. Thus she began to take me as a well-wisher and there created a good relation between us.
Family condition
My patient live with his family in Chittagong in his own home. At first phase of his married live he used to live in Dhaka. But after this long years and after losing his job and business, he returned to his permanent resident, and living in the building which his father build. He has two boys, older of them aged 24, and a student of degree. And his young son aged 20 is a H.S.C candidate. He has a daughter of 12 years, who is a student of class 5. He and his wife are used to stay in BIRDEM and his children had to stay in Chittagong for the long 3 months.
Social condition
Client came from a respective middle class family of Chittagong. He still enjoy respect from the neighbor and from the relatives. So he has a good reputation in the society.
Economic condition
My client used to work in a garments factory a long time ago. But after that, he started business of cigarettes. His business was to carry the cigarettes from factory to the whole sellers. But that business wasn’t profitable enough for running his family. After that he went for a job in a still mil in Chittagong. He was in that factory just before coming to the BIREDM for treatment. Now he is unemployed. His two son earn through tuition, and runs their pocket money. He earn some money by renting a room in his home, he also have some financial assistance from his 4 brother and 3 sister. Mainly that is the main source of his income.
Mental condition
My patient was very upset and worried about his physical condition as well as his economic condition. having money from the relatives was a matter of shame for his. But he is nearly unable to walk, for that there is no guarantee of returning to his normal life where he can earn easily.
Problem which I identified
- Mental unrest.
- Unable to walk.
- Uncontrolled diabetes.
- Tension of future economic disaster.
Problem solving process
For solving his problem, I followed two process which are important in social case work.
- Supportive treatment method.
- Correctives treatment method.
Supportive treatment method
Using this method I gave advice to him about how to control the diabetes, we had few open discussion about his physical problem, I behave demonstratively to let he know that the kind of problem she is facing Is not unique, and many way is still open f solving those problems. I shows his some of the patient of that word who were in more critical condition than him. I gave advise to follow the advise of the doctors.
I also gave him relative information about the self-employment for him, and about the social welfare department who are providing her a handy service to him and for his betterment.
Correctional treatment method
In this phase, I let him know about the perfect lifestyle, the family function, and disciplinary life for controlling this disease, taking the insulin regularly, and coordinate his family and to her lifetime disease.
I also discussed with his wife about the problem, and make her agree to follow the advise of the doctors.
Evaluation
It wasn’t a easy task to solve all the problem of my patient within the short period of time. I tried my best with my limited resources, and visited three time during my field work. I also meet him after his realease.
Application of Social Work Methods, Principles and Techniques in Field Work:
I have tried to do all my assigned duties during the field work practice. I have tried to use do the case studies in a disciplined way by the help of social work method and techniques. The assignments given my institute supervisor, I have tried to complete them well. I have handled the cases with the help of the basic methods of social work, social work helping process that means psycho-social study, diagnosis, Treatment Follow-up. Beside these I have practiced the basic and auxiliary methods of social work.
The total methods values principles and techniques I have practiced from the beginning to the end in my field work practicum are in the following-
Social case work:
Social case work consists of those processes which develop personality through adjustments consciously effected individual by individual between men and their social environment.
Social case work, which helps the individual client to affect better social relationships and a social adjustment that makes it possible for him to lead a satisfying and useful life.( Friedlander, 1968)
Principles:
As a trainee social worker I have used five principles of social case work in the problem solving process.
- Principles of Acceptance
- Principles of Communication
- Principles of Participation
- Principles of confidentiality
- Principles of adjustment of human behavior.(sarkar, 1987)
I have applied these principles to solve the problem of my clients.
I use the Principles of Acceptance in the level of first impression with the client every time. I tried to welcome them with a smile and friendly behavior. Using the principle of
Communication I was able to communicate with the client and I gave them chance to
Communicate with me, so that their problems could come out with a bloom.
I encourage the client to participate in their problem solving process, and ensure their decisions in their solving process.
Ensuring them that their personal information is completely safe and remain untold and will only be used in the departmental use, I had to use the principle of confidentiality. At last I use principle of self-determination in the different phases of my entire job.
“A person with a problem comes to a place where a professional representative helps him by a given process” the popular words of H.H. parlman was in my mind every moment of my job as a social worker, whenever I went to use social case work for solving the problem of my clients problem.
Methods and techniques of case study:
To study the problem of the clients, I have applied the following techniques and principles to apply social case work-
- I have used the theoretical knowledge of mental development, Behavior and social environment.
- I have also followed the principle of confidentiality about disease and other information of the clients.
- I have also followed the group dynamics approach of social group work.
- To know the sources of the problems of the client. I have followed the rule of psycho-social study. In this regard I have followed mainly the interview method and the techniques of interview method and they are- acceptance, observation, questioning, listening, talking, answering personal questions etc.
I have followed two kind of process a- social case work to solve the problem. They are-
- I have helped to get medicine, blood and others as supportive treatment.
- I have helped by counseling, advising, giving mental support to get a healthy and normal life as motivating treatment.
- Beside these I have also followed the principles of individualization and principle of self-determination.
- I have tried to apply principle of self-awareness also.
Social work administration:
Actually social work administration is the process of organizing and directing a social agency. The principles and programmes of social work are implemented by the help of social work administration.
Social work administration is the process of transforming social policy into social welfare services, involving the concomitant use of experience of modifies policy or method. (Kurtz,1957)
The knowledge of social work administration helps to complete various administrative activities. in this case various management process, such as the knowledge of planning, staffing, controlling, supervising, evaluation etc. are used.
The Experiences I gained as a trainee social worker
To attain the objectives of social work, the worker must have a profound knowledge in human nature, social relation, cultural values, environment, social changes and social institutions. Only the theory inside the classroom or in library cannot provide the worker this type of knowledge. It requires practical experience besides the theory to perform his duty perfectly.
I used my theoretical knowledge and gathered the following experiences:
- To receive a client as he/she is an important principle of social work. Using this principle I have learnt how to receive a client.
- Rapport is very much familiar phenomenon in social work. Using the theoretical knowledge on this subject I have learnt how to build up professional relationship with the stakeholders, clients and with their relatives as well.
- Social work believes in individual secrecy I used this principle and grows the confidence in the mind of my client and has found out various sensitive information regarding their disease.
- I have acquired the mentality to face any adverse situation.
- I have learnt technique how to study the client of different class.
- I have learnt how to deal with the key person of the agency.
- I have learnt how to counsel various types of clients.
- Motivation is also very much known topic in social work.
I worked as a field worker in BIRDEM for these working days. During this time, I have learnt something every day. I have verified and listed my theoretical knowledge in the light of practical situation. It was such a experiences that will provide me a lighting way in my future working life, these also provided me the experiences of working in a official environment, which was one of the big and valuable things I achieve from here.
As long as I was student, I was not much aware of the actual situation that our society is in. This practical training has given me practical knowledge of the issues and problems faced by the people specially the poor section of our society. I have tried to apply various methods of social work during fieldwork training.
Limitations/problems:
During this fieldwork training in BIRDEM I contrasted the following problems, which hampered my performance to a great extent.
- I had to take pain in building rapport with the service recipients due to their suspicious attitude. Some clients and stakeholders expressed vexation and declined to answer the question I asked them. As a result it was really difficult and painful task for me to study, diagnose and treat their problems properly.
- The environment was too much populated for give attention to the client, and service recipient.
- The behavior of the officers even the M.L.S.S. to the client is very hush. Some time I noticed client were crying. That makes me to think twice for dealing with the client.
- Due to time constraints of the clients I used to get very short time to take interview from them.
- Some service recipients declined to disclose the actual income, expenditure and real condition of their family, and this kind of attitude of the client was matter of disturbances for me.
- Due to fund crises I could not be able to provide material help to some poor clients. And these crises are getting more day by day. This may harm the whole system of providing of service.
- As a social worker I only had a identity card, this wasn’t enough for going everywhere I wished.
- The environment was so populated that I had few problems in following the principle of acceptance
- The behave from the doctors to social workers like us wasn’t up to the mark.
- In spite of the necessity of home visit and follow up I could not do so due to distance and lack of fund.
- As the duration of fieldwork was short I could not help some client completely within this short time.
- The agency even couldn’t provide us a better place to sit; sometimes we had to work in a populated place, and had to deal with the client by kept standing.
- The agency doesn’t have any criteria of how many trainee social worker should work in the agency in one time. In the mean time I had to work with another 22 social worker coming from different place.
- As social work is yet to get its professional value in our country so both the clients are not mentally prepared to receive the activities of social work which calls for problem in some cases.
Conclusion
As an apprentice social worker, the success of my social activity, as measuread in terms of helping clients or communities, is dependent on the helpful personnel of BIRDEM and nice organizational environment in which the work is carried out.In this respect BIRDEM is a leading institution, providing organised service, would be a pionner in this field. I am grateful to my honorable teacher and agency supervisor to give me the opportunity for such a rich experience. Moreover,I have gained insight and introduced with new terms of social service and its impact on people and the socity.I have also got introduced with the organization, its procedures, administrative process, personnel structure and programs.the experiences I have gathered from field work will greatly help for my future.
Last of all,I would like to express my hearty thanks and devoted reverence to my respective teacher and institute supervisor associate professor Md. Golam rabbani and my agency supervisor Mrs Dawlotunnesa for thire cordial guidance and inspiration,which I have received from the begining to the end of my fieldwork practice.