Main purpose of this research is to analysis Child Rearing Practices By Middle Class Mothers, here is a Sample Survey in Dhaka City. Other objectives are find out the nature of traditional child rearing attitude (system) of the middle class women of the city and examine the nature of practice of the child rearing knowledge of women of the city. Finally analyze the problems and barriers faced by the middle class women of the city.
Introduction
With impressive progress made in recent years, Bangladesh is one of few developing countries on track to achieve Millennium Development Goal 4 to reduce child mortality. Between 2004 and 2007 child mortality has fallen from 88 per 1,000 live births to 65 per 1,000 live births. However, despite this encouraging trend, neonatal mortality in Bangladesh is still high, accounting for more than half of all under-five deaths and more than two- thirds of infant deaths. An estimated 120,000 newborns die every year in Bangladesh. The share of neonatal deaths to infant mortality has increased over the period 2002-2006, largely because there has been little progress in preventing neonatal deaths. Poor neonatal health and under-nutrition of both mothers and children could affect the current success in improving child survival.
Bangladesh has one of the world’s highest rates of adolescent motherhood, based on the proportion of women under the age of 20 giving birth every year. 28% of adolescent women (age 15-19) are already mothers with at least one child and another 5 % is pregnant. The number of deaths among adolescent mothers is double the national average.
These high mortality rates are underpinned by the fact that 85 per cent of women give birth at home, most with unskilled attendants or relatives assisting. The low status of women, poor quality and low uptake of services are some of the reasons for this situation.
Because most births occur at home without skilled attendants, there is a high death rate of children under one month. Almost 80 per cent of neonates do not receive post-natal care from a trained provider within six days of birth. The first week of life is the most critical time for a newborn; three in four newborn deaths occur within the first week, almost 50 per cent of them within 24 hours, often at home and with no contact with the formal healthcare system (Lancet 2004). The major newborn killer is infection (52%) followed by birth asphyxia/unable to breath at birth (21%) and low birth weight/pre-term deliveries (11%).
Among the women and children who survive complications during childbirth, many are left with crippling disabilities that often cause them to be ostracized from the community.
All the above-mentioned information represents an overall scenario of the traditional or we can say the current child rearing system of middle class women of Bangladesh. Because these infant mortality and maternal health survey’s major proportion is occupied by the middle class women and children of the nation. This proposal is aimed to unearthing the current child rearing practice in the middle class women of Dhaka city.
Rationale of the Study:
Among the various problems of Bangladesh, infant mortality and child health issues are considered as one of the most important. This infant mortality and child health are mainly influenced by the poor knowledge and the traditional practice of child rearing system. We have enough publicity and facilities on child rearing system and infant health care conditions, but the traditional mentality of the middle class women in the country acts as the barrier to achieve the two gender related MGDs (Millennium Development Goals) “Reduce Child Mortality”, and “Improve Maternal Health” are yet to be achieved. The UNDP source says, in our country under five-child mortality rate is currently 53.8%, which is aimed to achieve 48% in 2015. Again the source says, the nation’s maternal mortality rate in per thousand women is 348, which is aimed to achieve 144 in 2015. But the current maternal mortality rate lower in tendency comparatively the last year.
Bangladesh has a strong breastfeeding culture. Almost all children are breastfed and continue to be breastfed until they are at least 2 years old. However, as shown in Figure 1, sub-optimal practices such as delayed initiation of breastfeeding, prelacteal feeding, non-exclusive breastfeeding, bottle feeding, and delayed introduction of complementary foods are common. Exclusive breastfeeding rates have shown little change in the past 15 years. Complementary foods are often inadequate in quantity and quality.
Figure 1: Infant and Young Child Feeding Practice in Bangladesh
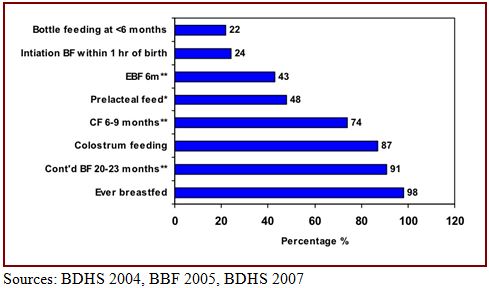
Research studies in various parts of Bangladesh report on knowledge and perceptions that affect breastfeeding practices. In a study among slum-dwellers in Dhaka (Haider et al., 2000), mothers introduced other foods before infants reached 4 months old because they thought breastmilk was inadequate, and they wanted to familiarize the baby with the bottle before returning to work. The perception of insufficient breastmilk was the reason given for early introduction of complementary foods in other studies (Haider et al., 1996; Haider et al., 1997). Factors that contributed to failure to exclusively breastfeed included domineering grandmothers, workload, or disinterest. Ethnographic interviews and focus group discussions in Matlab, Bangladesh, indicated that some women thought their breastmilk was inadequate because of their inability to eat, illness, or contraceptive use (Rasheed, 2007). This same study found that prelacteal feeding was more likely in home deliveries than in health facilities. Lack of knowledge was also associated with short durations of exclusive breastfeeding. In two studies in rural areas of Bangladesh, most mothers did not know the recommended duration of exclusive breastfeeding (Ahmed et al., 1999; Das and Ahmed, 1995).
Although childhood and infant mortality in South Asia has reduced substantially during the last decade, the rate of neonatal mortality in some countries of the area is still high. According to one source, 60% of all neonatal deaths and 68% of the world’s burden of perinatal deaths occur in Asia (Paul and Beorari, 2002). Further, although 70% of infant deaths occur during the first month of life, the policy-makers and health professionals in developing countries, until recently, neglected newborn care (Costello and Manandhar, 2000). On the other hand, this latter group of authors maintain that the principles of essential newborn care are simple, requiring no expensive high technology equipment: resuscitation, warmth to avoid hypothermia, early breastfeeding, hygiene, support for the mother-infant relationship, and early treatment for low birth weight or sick infants.
Newborn care often receives less-than optimum attention. Although, over the past 25 years, child survival programs have helped reduce the death rate among children under age 5, the biggest impact has been on reducing mortality from diseases that affect infants and children more than 1 month old. As a result, the vast majority of infant deaths occur during the first month of life, when a child’s risk of death is nearly 15 times greater than at any other time before his or her first birth.
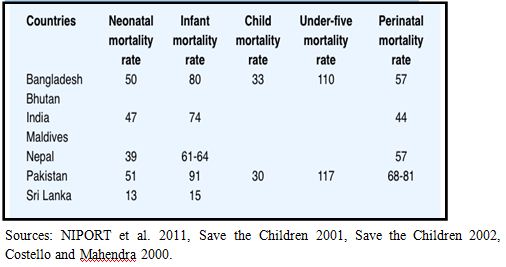
Unlike infant and under five mortality rates, reductions in neonatal mortality have been less in the developing countries and Bangladesh is a key figure among them (Darmstadt 2000). The average infant mortality rate worldwide has dropped from 95 per 1,000 live births in 1993 to 60 per 1,000 live births in 1995 (Costello, 1995; Stembera, 1990). But the progress in reducing perinatal and neonatal mortality in South Asia region has been distressingly low despite improvement in childhood and infant mortality rates in the last two decades. Table-1 shows newborn health status for countries in South Asia. It can be observed from the table that both neonatal and perinatal mortality rates are highest in Pakistan (51 and 68-81 respectively), followed by Bangladesh (50 and 57 respectively). The issues of perinatal and newborn infant health, therefore, require focused attention in South Asia.
Since 2000, UNICEF has been able to support a national programme for emergency obstetric care under the Women’s Right to Life and Health project. More recently UNICEF supported health facilities to provide improved newborn care.
Figure 2: Newborn health status for countries in South Asia
Health facilities have been equipped with necessary equipment for comprehensive emergency obstetric and neonatal care. Some facilities were also provided with laboratory facilities to enable safe blood transfusions. The equipment is regularly maintained and record keeping and reporting systems have been institutionalized.
In addition, doctors and nurses received emergency obstetric/neonatal care and anesthesia training. Laboratory technicians were trained to handle safe blood transfusions. Hospital staff was sensitized through training to women’s needs and concerns -including the issue of domestic violence to ensure that the rights and dignity of female patients are respected.
In the recent years, UNICEF adopted a comprehensive approach, with the aim of providing to all mothers and newborns a continuum of care -before delivery, during delivery and after delivery. This continuum of care is possible through better integration of quality maternal, newborn and child health care. UNICEF and other partners are also providing the Government of Bangladesh with technical and financial support to develop a National Neonatal Health Strategy and Guidelines. The strategy will set the programme directions in terms of operationalizing neonatal health care across the country.
But none of the above programs are practical enough to identify the actual child rearing system of the country. The policy makers often ignore the child rearing system and the practice of knowledge about child rearing. Without actual information about the child rearing system practiced by middle class women, who are the majority of the nation, it is not possible to achieve the MGDs of Bangladesh.
Foregoing study is intended to identify the real child rearing system practiced by the middle class women of Dhaka city. This is hoped that the study will clarify the necessity and importance of the knowledge on child rearing system practiced by middle class women to the future researchers.
Objectives of the Study:
Broad Objective: The main objective of the study is to find out the nature and condition of child rearing knowledge of the middle class women of Dhaka city and how they practice it.
Specific Objectives:
- To find out the level of knowledge of the middle class women on child rearing system.
- To find out the nature of traditional child rearing attitude (system) of the middle class women of the city.
- To examine the nature of practice of the child rearing knowledge of women of the city.
- To analyze the problems and barriers faced by the middle class women of the city.
- To explore the role of govt. and non-govt. organizations on providing child-rearing facilities to the city middle class women.
Hypotheses of the Study:
- The higher the educational status of the mother, the higher the knowledge on child rearing system.
- The neonatal health care problems may be reduced through proper knowledge distribution of child rearing to the mothers.
- The child cares knowledge and practice changes with the changes of socio-economic status of the family.
Review of Related Literature
Anu Rammohan et al. (2007) identified that; the excess female infant mortality observed in South Asia has typically been attributed to gender discrimination in the intra-household allocation of food and medical care. However, studies on child nutrition find no evidence of gender differences. A natural explanation could be that in environments of high infant mortality of females, the surviving children are healthier, so that child nutrition cannot be studied independently of mortality. In this paper, we use data from the 2004 Bangladesh Demographic Health Survey to investigate if there are any gender differences in survival probabilities, and whether this leads to consequent differences in child nutrition. We argue the importance of establishing whether or not there exists a dependence relationship between the two random variables – infant mortality and child nutrition – and in order to detect this we employ a copula approach to model specification. The results suggest that male children have a significantly lower likelihood of surviving their first year. However, conditional on survival, they have better height-for-age Z-scores. From a policy perspective, household wealth and public health interventions such as vaccinations are found to be important predictors of better survival and nutritional outcomes.
Fardaus Ara (2008) said, like other social sectors, health governance in Bangladesh is identified with poor and inefficient service delivery. Health care provision depends on efficiently combining financial resources, human resources, and supplies, and delivering services in a timely fashion distributed spatially throughout the country. To ensure good governance in this sector it is equally important that health services be delivered efficiently and health professionals are accountable to the public and government for their action. In Bangladesh, lack of voice and accountability; government ineffectiveness; low level of regulatory quality; weakness in establishing rule of law; lack of transparency and, corruption — all are impediments to good governance in this sector. This study highlights these core issues and at the same time recommends some policy prescriptions to ensure good governance in this sector and thus a healthy nation.
Charlotte Warren (2010), Every year, 120,000 newborns die in Ethiopia. In 2005 a national Safe Motherhood Community-Based Survey was carried out on behalf of the Family Health Department to explore community practices surrounding newborn health and care seeking behavior. To explore and understand health seeking behavior, and identify the positive practices surrounding care of the newborn. In-depth interviews and focus group discussions regarding newborn care practices were conducted with mothers, older women, men with young children, health providers, religious leaders and elders across Ethiopia’s 11 regions. Tradition recommends mothers and their newborns to stay at home for 40 days. The principle behind the practice, facilitates the period of rest and repair, establishes breastfeeding and is justified on the grounds that the mother and newborn are vulnerable to malevolent spirits. Perceptions of the causes of newborn mortality and morbidity are consistent with those relating to biomedical causes. Many complained of lack of accessible health care that in event of emergencies. Therefore they have to rely on traditional medicine as it is easily accessed, readily acceptable. When families seek care for their newborns, remedies from traditional healers are often preferred to skilled health workers because of cultural and religious beliefs, poor access to health facilities, (including distance and terrain) and financial barriers.
Since independence, health and fertility indicators in Bangladesh have improved substantially with the infant mortality rate and the total fertility rate both decreasing by about 50 percent. Despite these, the vast majority of the Bangladeshi population continues to suffer from poor health. Life expectancy at birth is about 61 years, one of the lowest figures in Asia. The under- five-mortality rate at 88 per thousand live births, which is six times higher than in Sri Lanka. The infant mortality rate in Bangladesh was estimated by the 2000 Demographic and Health Survey to be 66 per thousand live births and the maternal mortality ratio is estimated at 330 per 100, 000 births. A maternal mortality ratio of this magnitude is slightly less than that found in a few countries in the world and 100 times that of developed countries (ADB, 2005).
Less than 40 % of the total population has access to modern primary health care services beyond immunizations and family planning (Abedin, 1997 cited in Perry, 1999). Only 25% of pregnant women receive antenatal care, and only 14% of births are attended by someone with formal training (BBS, 1997c. cited in Perry, 1999). Malnutrition in Bangladesh is among the highest in the world. The extent of stunting and underweight are 45% and 48% respectively for children under five years of age, while anaemia is prevalent among 53% of pregnant women (CPD, 2003). According to the World Health Report 2006, Bangladesh in 2004 had 38 485 medical doctors, 20 334 registered nurses, 5 658 medical technologists, 5 743 public and environmental health workers, and 46 202 community health workers (CHWs). In spite of the progress made, Bangladesh has been identified as one of 57 countries with a critical shortage of the health workforce (doctors, nurses and midwives number below 2.28 per 1000 population). The nurses to population ratio of 0.14 per 1000 and nurses to doctors’ ratio of 1:1.85 are among the lowest in the world (WHO,2007).
The health care system in Bangladesh is a mix of public and private initiative. In terms of physical infrastructure, public sector is stronger than the private sector although in terms of coverage, the health care system of the country should be termed as a privatized one. Besides the private sector there are some NGOs, which also play a significant role in providing health services. All these institutions are managed and controlled under the policy guidelines of the government (Osman, 2004). The government’s efforts to provide health facilities at the various levels, though free of cost and managed by trained professionals, has however, not lead to desired level of use of the services. Primary health care services are greatly underutilized, despite repeated efforts by the government to improve these services (Jahan and Salehin, 2006).
Lack of voice and accountability, government ineffectiveness, low level of regulatory quality, weakness in establishing rule of law, lack of transparency, mismanagement by the government, lack of adequate human and financial resources, and, corruption – all are impediments to good governance in this sector.
Methodology of the Proposal
Methodology:
Methodology is the bone structure of a research. Methodology indicates the research techniques or tools used for conducting research. Methodology is the logical explanation of the research. Here the research steps are described along with logical explanation of choosing these tools and methods, assumptions and rationale behind them.
However methodology is the rational & theoretical perspective. It is mainly the combination of quantitative or qualitative method. This research is amid to be conducted by quantitative method.
Methodology of the Study:
One the other hand the Quantitative research deals with objective facts, focus on variables, a lot of cases instead of a few and specific cases, its subjective and value free. Here reliability is the key factor
I here in my research used Quantitative methodology for my research monograph. Quantitative analysis is an analysis of numerically coded data especially ordinal, interval & ratio data & often involving computation of statistical measures & tests of significance. As quantitative method is well developed & codified methods for data analysis, this method is used in this research. The other logical fact that favored to choose this method is that, this method is more easily replicable & less variable than qualitative method. It is highly developed & builds on applied mathematics & represents empirical facts in order to test an abstract hypothesis with variable construct. At the same time the limitation of qualitative research, i.e. unable to express numerically & unable to find the exact figure of the data & time consuming & money consuming matter encourage avoiding qualitative method & taking quantitative method for data collection. Moreover this method seems easier to conduct such a topic for research & that encourage choosing quantitative method.
Study location:
The research is intended to conduct on the middle class women of the Dhaka city. So the research’s study location is selected in the “Azimpur” of the Dhaka city.
Study Universe:
Study universe indicates the total number of subjects who have a quality to be chosen as my research sample. As I have conducted my research is in the azimpur of the Dhaka city so the total population of the area is considered as the study population or universe.
Unit of Analysis:
Unit of analysis or sampling unit is a well-defined, distinct and identifiable element or group of elements on which observation is made. An individual in a household may be a sampling unit, while the household in another case may be a sampling unit.
In my research as I wish to determine the knowledge and attitude of the middle class women of the city. So the women who have at least one baby are considered as the unit of analysis.
Sample Size:
The number of respondents or units contained in a sample is called sample size. This specific sample is interviewed and analyzed to conduct the research. There is a specific rule to estimate sample from population. M. Nurul Islam the professor of department of Statistics University of Dhaka have cited this rule in his book “An introduction to Research Methods” That is,
no = pqd2z2
Here, no = Desired Sample size.
P = Assumed proportion of target population estimated to have particular characteristic.
d =Degree of accuracy desired in the estimated proportion.
z = Standard normal deviate usually set at 1.96 for 95% confidence level.
q = (100-p)
In my research I have chosen 290 samples from my population get a result.
Sampling Procedure:
Sampling procedure refers to the specific system of choosing samples from the population. As I have referred earlier that, I had to conduct this research monograph with a low budget and man Power within short period of time, so I had no chance to collect a large random sample from a huge population.
More over I need to study with a specific categorical respondent who did have any good sampling frame to collect through random sampling. So I select Purposive sampling as my sampling procedure. This sampling needs such a researcher who has good knowledge about the population of the study.
Sampling Instrument:
For conducting a study every research methods have their own instrument of date collection. Data need to be consciously identified, carefully selected, methodologically collected &accuracy & precision are obviously important quality in research measurement.
In this study scheduled interview of survey method has been taken. This survey can be useful for descriptive, explanatory & exploratory purpose. This method is probably the best method in social research as it easy to collect empirical data with limited time & money. However this method is useful to collect authentic data from lower educated people like the respondents of this study by asking scheduled questions & writing them from the respondents. So in this study survey method with interview scheduled has been used.
Steps of Developing Interview Schedule:
- First I have indicated the variables need to be analyzed in my research.
- I have made sections in my interview schedule based on the Sections.
- I have ensured that all the variables of my research are included in the interview schedule.
- I have included the key points of research objectives.
- I have put appropriate code for close-ended questions.
- I made some open ended questions to know the opinion of my respondents.
Through these steps I have successfully collected necessary data from respondents and used in my research that support to test my hypothesis.
- Reasons of choosing Structured Interview Schedule:
- It is flexible than other quantitative data collection techniques.
- It helps to collect data from illiterate or respondents who are not able to answer in written form. As my respondents are selected from village and as they are women so I have greater probability to face illiterate respondents. So I chose interview schedule as my data collection technique.
- It provides best sort of data for quantitative research,
- Collected data can be best used in statistical analysis.
- This technique allows greater reliability and validity of collected data and reliability is the key in quantitative research.
- It helps researcher to make interactive relation with respondents and this interaction can help researcher to know more about his research objectives.
- Interview schedule provides all the answer asked to the respondent and no response problem is low.
- It allows controlling the data collection environment.
Data Processing:
Data processing is very important for quantitative research. The reliability is very much related to right procedure of data processing and analysis. I here in my research used two distinct way to processing my data.
To analyze the data collected from interview schedule I have used Statistical package For Social Sciences (SPSS) software. I have took a training from the “Department of Statistics” of University of Dhaka on the SPSS software and used to analysis the quantitative data of my research.
Limitations of Study:
I had to face some constraints to conduct my research. That’s:
- I have done this research as a partial fulfillment of my study of so I had not enough time to conduct the research. I had to do it within a limited time.
- I as a student had not any economic support from any organization. I had to conduct the research with my own money.
- I had to face some problems collecting information about malnutrition.
Theoretical Framework
The research topic ‘Child Rearing Practices By Middle Class Mothers’ is an attempt to identify the system and style of child rearing practiced in Dhaka city by the middle class women. Here the attitude of women or broadly the parents is the main goal to evaluate. The concept of parents attitude to child rearing is closely related to the theory of Diana Baumrind’s (1966) published in her first paper ‘Effects of Authoritative Parental Control on Child Behavior, Child Development’ where she describes three types of parents in our society and their different attitudes towards their children. The theory shortly can be described as follows.
The permissive parent attempts to behave in a non-punitive, acceptant and affirmative manner towards the child’s impulses, desires, and actions. She [the parent] consults with him [the child] about policy decisions and gives explanations for family rules. She makes few demands for household responsibility and orderly behavior. She presents herself to the child as a resource for him to use as he wishes, neither as an ideal for him to emulate, nor as an active agent responsible for shaping or altering his ongoing or future behavior. She allows the child to regulate his own activities as much as possible, avoids the exercise of control, and does not encourage him to obey externally defined standards. She attempts to use reason and manipulation, but not overt power to accomplish her ends.
The authoritarian parent attempts to shape, control, and evaluate the behavior and attitudes of the child in accordance with a set standard of conduct, usually an absolute standard, theologically motivated and formulated by a higher authority. She [the parent] values obedience as a virtue and favors punitive, forceful measures to curb self-will at points where the child’s actions or beliefs conflict with what she thinks is right conduct. She believes in keeping the child in his place, in restricting his autonomy, and in assigning household responsibilities in order to inculcate respect for work. She regards the preservation of order and traditional structure as a highly valued end in itself. She does not encourage verbal give and take, believing that the child should accept her word for what is right.
The authoritative parent attempts to direct the child’s activities but in a rational, issue-oriented manner. She [the parent] encourages verbal give and take, shares with the child the reasoning behind her policy, and solicits his objections when he refuses to conform. Both autonomous self-will and disciplined conformity are valued. [She values both expressive and instrumental attributes, both autonomous self-will and disciplined conformity] … Therefore she exerts firm control at points of parent-child divergence, but does not hem the child in with restrictions. She enforces her own perspective as an adult, but recognizes the child’s individual interests and special ways. The authoritative parent affirms the child’s present qualities, but also sets standards for future conduct. She uses reason, power, and shaping by regime and reinforcement to achieve her objectives, and does not base her decisions on group consensus or the individual child’s desires.