BRAC’S innovation in health: A case study
This study document and highlight the success stories of NGOs in health sectors, especially in BRAC health programs. This study is also share the level of commitment and initiatives of BRAC those were useful for brining innovations in health sector. It also examines the factors, approaches and strategies those were responsible for BRAC’s innovation in health sector.
BRAC Health Care Innovations Program intends to present and deliver comprehensive and worldwide healthcare services to the community people. Community Health Volunteer, familiar as ‘Shasthya Shebika’ in Bangladesh is the foundation of BRAC’s health programs. SS are female volunteers that are employed and trained by BRAC to give a variety of essential healthcare services to their communities. What is exclusive about BRAC’s approach is that, while these women can be regarded as volunteers they do not obtain remuneration. They are provided with financial incentives on the retailing of basic medicines and selected health commodities to their community. This sets BRAC apart from other health programs that rely on Community Health Workers and raises vital questions about the financial and programmatic sustainability of BRAC’s approach.
It is well known that relying on formal institutions to train health workers requires considerable time and financial investment. BRAC was the first organization to set up a Community Health Volunteer program in Bangladesh in the 1972s. BRAC addressed these matters by recruiting and training female community health volunteer. They are an impressive force in terms of their numbers, geographic coverage, and quick mobilization.
The BRAC Health Program operating model obviously relies on the successful recruitment, training, and retention of female community health volunteers. The rationale for BRAC’s approach is that community-based financial incentives of a volunteer community health workforce can attain broad program coverage and respond to community essential healthcare needs. It also provides earnings opportunities to its female volunteers in lieu of performance.
BRAC’s healthcare programs is the instance of low cost and simple equipment integrated within a development perspective could generate parallel results in comparison to high cost, sophisticated intensive methods.
The health impact of BRAC is closely shared to its approach: its partnership with those it serve up, its admiration for women, particularly poor women, its consideration to effective support, management and evaluation, and above all, its stimulating leadership. BRAC’s human resources and their partners trust that a better life is possible for all, and by their actions plan to become conscious this belief.
By recognizing the multidimensional nature of poverty, BRAC seeks a holistic approach to its programs. The comprehensiveness of programs acknowledges that improving the health of the people of Bangladesh cannot occur without development in all essential areas including education, economic, and social spheres in a strategic approach to counter act poverty through livelihood generation and sustainability.
General Introduction
Bangladesh has one of the most dynamic Non Government Organization (NGO) sectors in the developing world. The NGO sector works through a good working partnership with the government, and serves to fill the gap left empty space by government services.
BRAC is the NGO of success, spreading solutions around the development world. It is a global leader in creating hope for the world’s underprivileged people. It was started as a limited relief operation in 1972 in Bangladesh and has turned into the largest development NGO in the world. It attained this apex position by innovation, governance and commitment to success.
In healthcare, the word “innovation” has typically been meant for the improvement of new therapies, drugs, or medical devices. It means how can we reduce costs and add to value, get better patients’ experiences and outcomes, create healthcare something that people can have access? With GO and NGO collaboration, Bangladesh has made huge development in healthcare in the last four decades after independence. In the 1980’s, when immunization coverage was 2 per cent, the shared responsibilities and activities of BRAC and the government improved the grade to 70 per cent within the last 4 years. The current status is “most children are protected from preventable disease through high immunization coverage, with 84 per cent of children aged 1-2 fully vaccinated.
By BRAC’s collaborative program with government, cure rates for TB go over 90%, among the highest in world. BRAC has enormous innovation with success stories in health sector with cooperation of government of Bangladesh. It is time to learn from BRAC by critically investigate BRAC’s innovation in health sector.
Rationale of the Study
In socio-economic perspective of Bangladesh, NGOs have a significant position and is playing an important role towards nationwide development over last 43 years. NGO sectors influence the social development through teamwork with collaboration of government. Effective teamwork is useful to both the parties to develop the society.
Teamwork among health care providers can generate synergetic result. At present, BRAC is the world biggest NGO considering number of employees. It has huge innovations and success stories in social services to alter the life story of poor. Sharing these innovations, it is expected that the policy makers, researchers, academics, community leaders, GO & NGOs executives will be benefitted. It will also add value to academic literature, scholars to review the recommendations and apply them to other NGOs and government to evaluate their effectiveness.
Objectives of the Study
The objectives of this study are:
- To document and highlight the success stories of NGOs in health sectors, especially in BRAC health programs.
- To share the level of commitment and initiatives of BRAC those were useful for brining innovations in health sector.
- To examine the factors, approaches and strategies those were responsible for BRAC’s innovation in health sector.
Research Questions
The Principal research question of this dissertation is:
What are the contributions of BRAC’s innovation in health sector?
To answer the principal research question, the following sub-questions will supplement the question.
- What kinds of innovations were used in BRAC’s Oral Therapy Extension Program? What initiatives were taken to bring those innovations?
- What were the major innovations in BRAC’s Directly Observed Treatment Shortcourse (DOTS) for TB strategy? How those innovations were implemented?
Scope of the Study
Learning from BRAC’s huge innovations are the main scope of this research. BRAC’s huge research and innovation in different social sectors have vast scope of learning for NGOs, GO and other organization. Due to time constraint, three research objectives are taken of this study. BRAC has an vast success to control the diarrhea by oral therapy extension program. In 1980s, BRAC spread out the home base oral saline preparation formula of diahrroea patients by salt and raw sugar (gur).This program is now closed due to vast advertisement and commercialized production of oral saline. So, for study of innovation of oral saline program, secondary data, case study and contend analysis method are used. On the other hand, for the ongoing DOTS (TB) program, primary data as well as secondary data are collected by interview method and published documents.
Content analysis and case studies is also followed for the study.
Limitations of the Study
The study is a part of the Masters in Governance and Development (MAGD) Program.
For this dissertation, only three objectives are selected. Although BRAC is serving all 64 districts of Bangladesh, only Savar upozilla of Dhaka is selected as study area. BRACs social innovations i.e. Oral Saline and DOTS (TB) program are selected as case analysis.
Apart from the data collection, key informants and direct stakeholder like patient primary data and secondary sources data are used.
Research Methodology
Research methodology is the lessons used to collect information and data for the purpose of making dissertation decisions. This chapter presents the methodology have applied for collecting, processing and evaluating data. It structured research approach, research design, research methods and techniques used for data collection and data analysis. For the purpose of this study no single methodology will seem to respond to the research need rather a combination of methods will be of useful for bringing desired level of methodological achievement. Accordingly the following three methods will be used here:
- a) Content analysis
- b) Focus group discussion
- c) Case-study
The methodology is largely used in this study is based on secondary data through content analysis from reports, reviews, books, journals, existing policy and practices. The primary data is mainly relied on the focus group discussions with key informants and the stake-holders. There is also be some pictures of real life experiences which is exposed during the survey to authenticate the study by exposing the reality of the BRAC health innovation of Bangladesh.
Content Analysis: “Content analysis method critically and objectively reviews the published or printed facts, figures, opinions, observations, generalizations in the light of its content value” (Aminuzzaman,1991). Content analysis is used to gather secondary data which is collected from different relevant publications, dissertations, books, journal, articles, research reports, government publications, rules regulations and acts and websites to understand the functions of the BRAC Health sector. A literature review is done accordingly.
Focus Group Discussion: A focus group discussion is an approach to collect people from related backgrounds to discuss a specific topic of interest. The group of participants is guided by a mediator who introduces topics for discussion and helps the group to take part in a lively and normal discussion among the group. In bridging research and policy, it can be helpful in providing an insight into different views among different groups involved in the change process, enabling the process to be managed more efficiently. It is also a good method to use prior to designing questionnaires.
Case Study: Thomas offers the following definition of case study: “Case studies are analyses of persons, events, decisions, periods, projects, policies, institutions, or other systems that are studied holistically by one or more method. The case that is the subject of the inquiry will be an instance of a class of phenomena that provides an analytical frame, an object, within which the study is conducted and which the case illuminates and explicates.” The case study can be defined as a research strategy that investigates a phenomenon within its real-life circumstance.
Source of Data
Both primary and secondary data is collected. For representative data, stakeholder’s like patient’s direct interview and key informant’s like local representative’s interview has taken by telephone. Accordingly questionnaires (annexure I & II) are prepared to collect data. All primary data are collected by author himself from key informants and patients. It was provided interviewees the opportunity to review the transcripts and make correction.
Content analysis was done from different documents, articles, internet relating to this study.
Sample Area
For data collection of this study, Savar upazila in Dhaka district is selected. There are 12 Union Parishads under Savar upazila. They are Savar, Birulia, Dhamsona, Simulia, Asulia, Yearpur, Vakurta, Pathalia, Bangaon, Kaulia, Tetuljhora, Aminbazar. Data are collected from every Union of Savar Upazila. The map of Savar upazila and location of Savar upazila in Bangladesh are shown:
Figure 1: Map of Savar upozila (Not in scale) Figure 2: Map of Bangladesh (Not in scale)
For best representative primary data collection, it is considered that Savar Upozila is divided by administrative 12 unions, and from each union’s key informants and TB patients, 6+6 numbers data are collected respectively. Secondary data are collected from various sources like internet, national and international publications, research organizations reports etc.
Literature review
BRAC as an NGO
At the very beginning BRAC was known as the Bangladesh Rehabilitation Assistance Committee and then as the Bangladesh Rural Advancement Committee which was initiated in 1972 by Sir Fazle Hasan Abed in the district of Sylhet, Bangladesh. It started with a small-scale relief and rehabilitation project to help returning war refugees after the Bangladesh liberation war of 1971. In 9 months, 14 thousand homes were rebuilt and several hundred boats were built for the fishermen, medical centers were opened and other necessary services were ensured. When the first phase of relief work was over, BRAC turned in the direction of long-term development necessities and re-organized itself to focus on the make powerful of the underprivileged people, particularly women and children at December 1972.
At present, BRAC is the world’s largest NGO. It has breached the borders of development standard, and indicating that poverty can be pushed back drastically if it is deal with directly. It has shown that poor, completely insolvent, women in a conventional muslim society can learn, earn, and direct. It has also shown that enterprise, sound business principles, and the market can be powerful allies in the combat against poverty.
BRAC has showed that a benevolent organization need not be soft, tiny, or immaterial. It has broken the borders of small, turning little experimental efforts into huge enterprises. The enterprises are staffed almost exclusively by thousands of poor villagers and whose own drawbacks were once labeled by short of knowledge, sick health, separation, and horror (Ian Smille, Freedom from Want).
Social Innovation is important to success in addressing a variety of needs with so little resources in society. The guidance of BRAC promoted new approaches and constantly asking for verification of both impact and sustainability. BRAC widely examined and then documented its experiences in close cooperation with those it served which is based on the daily meetings that took place each evening to share the experiences of the day. The outcomes were in turn shared with those who afforded funding for BRAC’s efforts, enabling them to estimate the impact of their support. Thus fund-raising became a matter of recording and disseminating the lessons of development.
Now BRAC is functioning in all 64 districts of Bangladesh, with over 7 million microfinance group members; 37,500 non-formal primary schools and more than 95,000.
Shasthya Shebika (health volunteers). BRAC is the largest NGO by number of staff employing over 120,000 people in over nine countries across Asia and Africa. BRAC functions various programs such as those in health, banking, microfinance, education etc. It is about 80% self-funded through a number of business enterprises including a dairy, bank, food project and a chain of retail handicraft stores. It has offices in 14 countries all over the world, including BRAC USA and BRAC UK.
.
BRAC Health Program
Public Healthcare: It was found by BRAC that there were not enough hospitals in countryside. Even if it could build, there wouldn’t be sufficient trained staff in Bangladesh. Instead BRAC found a local woman in each village area if trained her on all of the common diseases can carry on role in rural health service. These women were not paid by BRAC. They receive free training and BRAC wholesale medicines/contraceptives to them. They could sell to her patients/other members of her society. This process increased the trust of the villagers in the solution. It also allow early intervention and increased likelihood of completing the full drug course for diseases such as TB (Freedom from want, Ian Smillie).
BRAC Health has reached the under-privileged and deprived community through volunteer village women or Shasthya Sebika (SS) by and adopted a door to door service delivery approach. To reduce the income-erosion consequence of sickness and helplessness of the poor households, BRAC incorporates Essential Health Care (EHC) activities with its microcredit-based poverty-mitigation involvements. The EHC brings preventive and basic curative health services to the villagers through SS who is willing to provide voluntary services, and fit for the society. The SSs get four weeks fundamental residential training backed up by usual monthly refreshers. For programs such as DOTS, community-based ARI, or safe motherhood etc the SSs are given extra training. Each SS wraps around 250 households, and makes at least once a month appointment to the households. During these appointments, they rendering health, nutrition and family planning significances, inspire to install tube-wells and hygienic latrines, make out and documented pregnancy cases, identify TB suspects for sputum test. They also present treatment for common illnesses and sell health commodities. They work on unpaid basis but make some income from the sale of health commodities. Careful assortment, training, encouraging supervision, functional recommendation relation and performance-based motivations are main factors responsible for the sustenance of the SS model.
Sound health is to be attained by better medical, cleanliness and sanitation programs. It usually designed in a different place even if the collaboration of the community is earnestly required. The approach is largely top-down, even if covered by the fist being in a kindly, helpful and co-operating adore. The kind of thing dealt with in Health Transition Review and in the Forum in this issue does not come into view. A little appears about individuals’ behaviour, inspiration and health attitude, and nothing on the locus of duty, even if there is much about collaboration and galvanizing of society effort.
Many of the self-help society projects focus on issues that create better atmospheres. One wishes that shapes would substantiate the last hypothesis (R. John et al,1993).
DOTS (TB) Program: BRAC has created entrance to life saving diagnostics and treatment for hundreds of thousands by the Direct Observed Treatment-Shorts (DOTS) which is a community based TB control program. For over 25 years, health volunteers (SS) has brought services to the doorsteps of patients. From organizing movable outreach to collect sputum samples for diagnosis to implementing a bonding system to make sure treatment compliance, BRAC’s experience demonstrates how programmatic innovation and sound management methods can enable an organization to attain some of the highest cure rates while operating at unprecedented scale (May M.A., et al 2011).
TB has been a main public health apprehension for Bangladesh for last few decades. BRAC started the tuberculosis control program in1984 in one district as a pilot basis. In 1994, BRAC became the first NGO in the country to sign a memorandum of understanding (MoU) with the government to spread out DOTS services across the country. BRAC also became a principle recipient (PR) of the Global Fund to Fight AIDS,
Tuberculosis and Malaria (GFATM) together with the government. The aim of the program is to lessen the morbidity, mortality and transmission of TB until it is no longer a public health problem (www.health.brac.net).
Bangladesh implemented the internationally suggested DOTS strategy in 1993. Through the joint venture, DOTS services were made accessible to all sub-districts by 1998 and country attained 100% DOTS coverage by 2007. After two decades of working with joint venture, the partnership has grown and established as engine to achieve the country target in line with the global plan. It is now providing a well-built technical stage to generate political support and permit the country fighting against TB successfully. Now BRAC and under its leadership other 43 NGOs are collaborating with National TB Control Program (NTP) in providing TB services to practice and enhance completion of DOTS, increase case uncovering by engaging all health care providers (Rashid M. M, 2015).
SS executes a well-tested, community-based approach for increasing and sustaining TB case detection and treatment. During household visits, SSs ask simple questions related to suspected TB cases (based on symptoms). When a suspected TB victim is identified, the SS motivates the person to be tested at a nearby government facility and explains the dangers that TB can pose to the ill person as well as the rest of the family members. She then follows up with the patient to determine the test results and give advice accordingly. BRAC is contributing in combined resource mobilization, implementation, capacity building and health scheme strengthening. To strengthen the National TB Control Program, BRAC is also engaging diverse care providers to augment the TB control. As for BRAC TB control program, SS is the frontier care givers who freely serve the TB patients. These volunteers are providing services through community mobilization, identify and referral of presumptive and ensuring Directly Observed Treatment (DOT).
Diagnosed TB patients are given DOT by SS, generally at her house, under the supervision of field level employees of BRAC and a government. They are playing a pivotal position of connecting individuals with TB control services which dynamically contributes in the achievement story of national TB program. BRAC involves in sensitizing the community on TB prevention and utilizing the existing healthcare services through its varied activities. BRAC also work in the aforementioned areas but also for high threat congregate settings such as prisons, combined military hospital and academic medical colleges. BRAC regularly checks the program performance of BRAC itself and also partner NGOs; ensures timely reporting to the government; continues the quality of services; distribute the fund to partner NGOs; develops capability to malaria staffs, coordinates between different stakeholders such as government’s different agencies, WHO, NGOs, private sectors, local bodies etc (Rashid M. M, 2015).
BRAC cares for about 150,000 TB patients per year. National TB case notification (Figure below) and treatment success rate have increased considerably; that is an outstanding attainment of partnership. The performance of BRAC DOTS is shown:
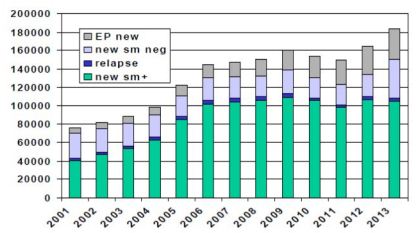
Figure: Number case notification of TB Patients in Bangladesh (Source: Rashid, M.M,2015)
Oral Therapy Extension Program: In Bangladesh, about one third of the total children are passing away burden due to diarrhea (Victora et al, 1993). Each year, a rural child suffers on average from 4.6 episodes of diarrhea, from which about 230,000 children die (BBS, 1996; Mitra,1994). A Simple Solution is a tale of how a medical technology was adapted, revised and presented to ad illiterate community through house-to-house health education by a health care group of dedicated health workers. Through a decade of persistent work, the entire BRAC organization started this motivated program, and despite of all uncertainty from the global public health community, carried the knowledge of oral therapy into every residence in Bangladesh. Never earlier, or since, has a public health effort of this passion been tried. Never before has health education been provided under such exact and cost effective circumstances with regular monitoring and evaluation; resulting in improved execution at progressively lesser unit cost (Cash R. A, 1996 ).
O.R.S. refers to oral rehydration solution, a simple but life-saving drinking water, salt and sugar formulated in the late 1960s by American and Bengali physicians and researchers working in Dhaka, Bangladesh. Unlike saline intravenous drips to care for severe dehydration from diarrhea, O.R.S. was cheap. It did not require special, hygienic equipment and could be made at home. The potential of O.R.S. in underprivileged countries was enormous (www.brac.net).
Oral rehydration early program monitoring showed that most mothers could prepare a safe and useful solution, but that its apply was fewer encouraging. BRAC message promoting lobon-gur solution (LGS) for all types of watery diarrhea was understood by the people to be of mainly use for rigorous watery diarrhea (Vaughan J P, 1988). Oral Rehydration Therapy (ORT) is being commonly supported in developing countries. But the socio-cultural aspects of diarrhea are often poorly investigated prior to planning the programs. Since 1980, the BRAC as an NGO has encouraged a home-made ORT solution for use in all diarrhoeal episodes called LGS which is made from household lobon (salt) and gur (unrefined sugar) using the ‘pinch-and-scoop’ system. One mother per household is trained in its homework and use during a half-hour home visit. By late 1986, over 7 millions of Bangladesh’s 16-million households had been visited.
BRAC SCALE-UP in ORS
Inspired by the “Year of the Child” (as proclaimed by UNESCO in 1979), BRAC leadership came to a decision to move the organization’s focus from family planning to treatment of childhood diarrhea. The organization had recently scaled up a credit program and considered that an ORS program would be straight-forward to get bigger because it only engaged disseminating education; it did not rely on any external factors or sectors.
In spite of the reality that NORP was also working in ORS, the government of Bangladesh granted BRAC’s application to start a project. BRAC decided against using static health centers because they felt that they were not numerous enough, the rural poor did not have sufficient access to them, and the organization did not want to rely on the government. Instead, they began a program to teach mothers to make their own ORS, called Lobon-Gur (salt-sugar) Solution (LGS), at home. First piloting the scheme in two villages, BRAC employed teams of female health workers with one male supervisor and, importantly, one cook. The female team went door-to-door teaching mothers how to get ready the solutions using pictures and demonstrations. After some revisions, BRAC make a decision on a 7-element message that they need each mother to learn (Chowdhury and Cash 1996). The seven points to remember, from “A Simple Solution” are as:
- What is diarrhea? (other names: dood haga, ajirno, amasha and cholera)
- Symptoms of dehydration
- Simple management of loose motions
- Preparation of oral saline
- Administration of oral saline
- Advice to maintain nutrition through illness
- Prevention of diarrhea
The payment method for these volunteer teams was incentive-based. Approximately 10% of the homes visited by each woman would be sampled, and their income would be based on how well each mother remembered how to put together ORS (Chowdhury and Cash,1996). The women volunteers also brought ORS packets with them for sale (Rohde 2012).
After achievements in the pilot project, the program was nationally scaled-up in three phases. Each phase used the same replica and expanded into new regions. Preliminary supervision found that although knowledge of LGS was high, real use of the treatment remained low. BRAC identified two causes for this: sugar was often out of stock in the home, and men had not been sufficiently involved in the procedure. To address these matters, they ensured that mothers knew they could use different sorts of sugars, and began marketing attempts to reach out to men at mosques and similar meeting places.
They also began educating kids at schools, educating community doctors, and advertising through publication and radio media. The third segment of the program finished in 1990. About 1,20,00,000 mothers were trained from 1980 to 1990 (an estimated 46% to 63% of women aged 15-49 in Bangladesh at the time (US Department of Commerce 1993)).
Since the ending of the scale-up, BRAC has upheld to sustain ORT and ORS by training CHWs in diarrhea management throughout Bangladesh (Rohde 2012). The Manoshi Project: The Manoshi Project at BRAC presents community-based maternal, neonatal and child health services for 6.9 million town slum dwellers in 10 cities in Bangladesh. At the beginning of the projects in 2007, this population had high maternal and neonatal mortality. At 2008 service population survey exposed a maternal mortality ratio of 294 per 100,000 live births and a neonatal mortality rate of 43 per 1,000 live births in 2008 correspondingly (Manoshi Performance Report, 2012). A majority of women (86%) gave birth at home, and only a quarter obtained the suggested antenatal and postnatal care (Moran et al., 2009). This population is hard to serve since its members are frequently short-lived, lack suitable addresses, and face intimidating healthrelated challenges such as overcapacity, poor hygiene, severe poverty and indecision to look for medical care (Moran, et al., 2009). Even governments that prioritize serving the poor often have complexity creating policies that can effectively attain this highly mobile, dense, socio-culturally heterogeneous population (Khatun, et al., 2012; More, et al., 2012). The purposes of BRAC’s SS, SK and UBA are described:

Table: Service delivered by the CHWs of Manosi Program
Manoshi users are aware of the advantages of birthing huts including privacy, availability of trained birth attendant, referral linkage, and free of charge care. These are not the only reasons behind the decision to deliver at the birthing hut. The immediacy of the birthing hut to the home and unavailability of persons to accompany the women during labor pain were also among the causes that led women to deliver at birthing huts. Non-use of the birthing hut by women is related to the need of commonly accepted procedures (oxytocin injections and saline infusions) rather than the CHWs role. All service receivers accept and trust the CHWs. It is important that in the future all efforts are made to preserve and improve the communal capital created by the CHWs in the slums.
Non-Communicable Disease (NCD) Program: Non-communicable diseases (NCDs) normally occurring amongst the people of 35 years and over, require a large quantum of health and social care, irrespective of socio-economic status. Most NCDs are chronic debilitating disease associated with a range of severe complications. Bangladesh has a big number of people living with NCDs. BRAC is also going to take on NCD pilot initiatives in 3 sub-districts of two districts (Narayanganj and Narsingdi) under EHC and 8 sub-districts of 5 districts under Leeds University COMDIS study project. Initially there will be screening, referral and follow up of hypertension and diabetes patients in the society (www.health.brac.net).
Vision Bangladesh Project (VBP): This project is undertaken in collaboration with the government health sectors under the leadership of the Civil Surgeon. All BRAC staffs are trained in prevention of blindness at the involvement areas. The activities include dissemination of eye health message, patient finding, referral to eye care facilities and report on of the patients. BRAC staff mobilizes the community people through diverse forums to attend Patient Screening Program (PSP) for eye care services. The community health workers are trained to identify suspected cataract patient and perform the activities by visiting houses. They refer suspected patients to the PSP for screening. The identified cataract patients are referred to specially selected eye hospitals. The operated patients are followed up at residence. If any complications happen, respective eye care hospitals are urgently informed for suitable management of the patients. Local government stakeholders are also connected in the program (www.health.brac.net).
Malaria Control Program (NMCP): The Government and BRAC collaborative approach is a well-established and nice example of Public Private Partnership (PPP) model. It is welcomed at national and global levels. Malaria is a major public health problem in some areas of Bangladesh, mostly in 13 districts in the north-east & southeast areas which boundary of India and Myanmar. Among them are the Chittagong Hill Tracts (CHT) districts which extremely endemic and Cox’s Bazar which is fairly endemic. The other districts are categorized as little endemic areas as less numbers of cases have been reported there. Irregular incidences happen in other parts of the country.
The NMCP produced an effective joint venture with a consortium of 21 NGOs led by BRAC. This partnership has leveraged the program and increased the access to malaria treatment, prevention and awareness raising activities inside communities, including the hard-to-reach parts. In partnership with NMCP, BRAC successfully secured a funding from the GFATM to strengthen and spread out national malaria control activities to all endemic districts working directly and throughout other NGOs. BRAC is directly executing malaria control activities in all districts of CHT and through 20 partner NGOs in other districts which are supervised by BRAC. To reduce the general burden of malaria (morbidity and mortality) by 60 percent from baseline year 2008 in 10.9 million populations in 13 high endemic districts of Bangladesh by 2015 (www.health.brac.net).
During home visits, the CHV identifies suspected cases of malaria and refers the patients to the adjacent government health centre. She follows up to determine test results and see if the patient is taking their anti-malarial medication. A relative of the patient is place in charge of supervising the drug eating according to their prescription. The CHV then conducts a follow-up visit to make sure the patient’s improvement and to make sure that the patient has not developed more complications. CHV keeps records of this information in her home visit register. CHV are distributing home-based management of malaria as part of the Child Survival Program of the Ministry of Health, Government of Southern Sudan.
Maternal, Neonatal and Child Health Program: BRAC have initiated maternal, neonatal and child health (MNCH) programmers’ in 2005 as a pilot project and has been scaled up to 11 city corporations and 14 rural districts in cooperation with the government, UKAID and Australian High Commission. With the active engagement of community health workers and birth attendants, BRAC ensure high coverage of antenatal and postnatal care while supporting skilled birth attendance (www.health.brac.net).
Reproductive Health Care: BRAC expects to progress reproductive health care awareness and service utilization. To fulfill this objective, Community Health Volunteers (CHVs) identify pregnant women during their household visits and notify the Community Health Worker (CHW). The CHWs perform antenatal health checks Counseling and Testing (VCT) for HIV/AIDS, and Preventing Mother to Child Transmission of HIV, in the residence, raising consciousness of pregnancy care and pre-natal risk symbols. The CHV maintains a check on whether her the patient have taken their Tetanus Taxied (TT) vaccine or not. She also increases awareness of the importance of voluntary (www.health.brac.net).
Family Planning: CHVs mobilize and inspire women to use contemporary methods of contraception by providing clients with birth control pills and condoms. For other shortterm and/or permanent methods, couples are referred to government primary and secondary healthcare facilities (www.health.brac.net).
Community Health Initiatives: BRAC is highly concern about community health initiatives. A multi-pronged approach to community health education by offering community health forums on subjects like malaria, TB and HIV prevention, maternal health, family planning and sanitation by BRAC (www.health.brac.net).
Basic Curative Services: CHVs are trained to detect and take care of some basic ailments such as diarrhoea, dysentery, cold, anemia, ring worm, scabies, hyperacidity and angular stomatitis. They refer patients with suspected conditions to local public and private health facilities. CHVs make a small profit by selling over-the-counter medicines to patients (www.health.brac.net).
Nutrition Program: Malnutrition is a main public health concern in Bangladesh. To concentrate on this problem, nutrition program has been working at home and society level for creating consciousness on nutrition by BRAC. BRAC’s SS and nutrition promoters visit homes in their societies and present counseling, coaching and exhibition.
Moreover, they offer Community-based Management of Severe Malnutrition (CMAM) service to mother and child of 6 to 59 months who are influenced by practical accurate malnutrition by providing additional food. Nutrition program creates consciousness about teenager girls’ nutrition and encourages mothers and family members about many matters like intake of healthy and various sorts of food, early initiation of breast feeding, exclusive breast feeding till 6 months, breast feeding for as a minimum two years and initiation of complementary feeding after six months. Moreover, to prevent child malnutrition and anemia, micro-nutrient powder sachets are allocated under maternal, infant and young child nutrition (MIYCN) home fortification program (www.health.brac.net).
MDGs and BRAC
UNDP are continuing press on to meet the Millennium Development Goals (MDGs), eight anti-poverty goals that the world committed to achieving by 2015. Bangladesh walks in reaching the goals of MDGs, and BRAC’s multidimensional programs are helping women to attain the more optimal health position wanted by the MDGs 4 and 5.
MDG 4 – Reduce Childhood Mortality
Prevention of diseases such as measles, poliomyelitis, and diphtheria–concurrent with widespread use of ORS for diarrheal diseases is successful. It has radically reduced childhood mortality and morbidity. This success is also due in fraction to the slight i) data as of April 2005 ii) the under-five mortality rate markedly vary according to socioeconomic position and disproportionately have an effect on the poorest. As of 2000, the rate of the poorest fifth of the population was 140 per 100,000 live births, 106 for the middle fifth, and 72 for the richest fifth (DHS Survey Year 1999/2000) increase in the number of births attended by trained health personnel from 5% in 1990 to 13.2% in 2004.
During the same time period, immunization against measles increased from 65 percent to 77 percent for children one year of age, though since among diseases that can be eradicated through immunization, measles is the leading cause of child deaths, this improvement is still under expectations.
A few of the challenging issues that must keep on to be addressed include neonatal and perinatal care, malnutrition, as well as particular targeting of un-reached and underserved populations. Though advancement has been made, there is still much work to be done to enter at the below five mortality rate goal of 50 per 1,000 live births by 2015 and this future progress is also dependent upon the social, cultural, and economic progress in the country (Muhiuddin Haider, 2007).
MDG 5 – Improve Maternal Health
To achieve this MDG, Bangladesh must drastically reduce its maternal mortality ratio (MMR) which stood at 574-850 deaths per 100,000 live births in 1990. In 2000, recent data has shown that progress has been made in the reduction to 320-400. To reach the goal of 143-213 deaths per 100,000 live births by 2015, the decrease will have to take place at considerable rates, and to address this, Bangladesh looks for to increase the proportion of births attended by skilled health personnel to 50%, and decrease the total fertility rate (TFR) to 2.2 per woman by 2010. It is a reality that ensuring ‘Good Health for All’ is a huge task. As a result of the changing geo-political conditions over the last few years, the interface between the government and the NGOs has increasingly been playing a corresponding function in bringing about constructive changes and thus in achieving the Goals of MDGs and national goals as well (Muhiuddin Haider, 2007).
BRAC’s Role in the Healthcare Sector of Bangladesh
Just after the Liberation War, in effect to the continuing difficulty of disease and illness within the population, health sectors were included into BRAC’s. It’s development interventions begin to hold up community level healthcare services and health education programs. BRAC’s healthcare programs summarized that low cost and simple technology incorporated within a development framework could generate similar results in compare to high cost, sophisticated thorough methods. This thought towards a sustainable health care system through dynamic community participation has remained constant throughout BRAC’s continuing health interventions. BRAC’s Health Program come together promotive, preventive, curative, rehabilitative healthcare. It focuses on improving maternal, neonatal and child health, fighting communicable diseases and ordinary health problems. BRAC’s Health Program is the result of an integrated approach, including some interventions to present a health service. It hold ups human development and works in joint venture with its comprehensive approach to development. The main areas of BRAC health program are: essential health care; tuberculosis and malaria control; maternal, neonatal and child health; family planning; immunization; health facilities and limb and brace centre (www.health.brac.net).
BRAC’s Approach in healthcare services
An awareness of the changing health needs, cost effectiveness, adaptation of technology, sustainability and delivery through partnerships with communities and government are main features in BRAC’s approach to providing healthcare to poor inhabitants. BRAC has accepted an epidemiology – experimentation – expansion assessment model to build up and deliver the program. Lessons learned from own experiences in public health, Oral Therapy Extension, Women’s Health, Reproductive Health and Disease Control programs, have enabled BRAC to expand sustainable and accessible health care to more that 100 million people across Bangladesh (www.brac.net).
BRAC innovation in health sector
BRAC Health Care Innovations Program (B-HIP)
B-HIP aims to present and deliver comprehensive and universal healthcare services to the society people. B-HIP structure and design are mutually being explored by James P Grant School of Public Heath, BRAC University and BRAC Health Program. The program plans to cater health insurance products to the less privileged people, thus, ensuring entrance to healthcare services to everyone (www.health.brac.net).
The Center for Health Market Innovations (CHMI)
CHMI supports programs, policies and practices that produce quality health care delivered by private organizations inexpensive and accessible to the world’s poor. Managed by Results for Development, CHMI runs through Regional Partners around the world and accepts support from the Bill & Melinda Gates Foundation, the Rockefeller Foundation, and UKaid. Building on the achievement of CHMI, Results for Development (R4D) initiated the Center for Education Innovations in 2013 to enhance access to quality, affordable, and equitable education. Following this achievement, R4D initiated the Social Accountability Atlas in 2015 to drive a boost in the quantity and effectiveness of civil society-led efforts to supervise and advance public spending and service delivery across divisions. Details on over 1,400 innovative health enterprises, nonprofits, public private partnerships, and policies can be found in CHMI’s programs records (www.healthmarketinnovations.org).
Research and Evaluation Division
BRAC set up a Research and Evaluation Division (RED) in 1975 to analyze and evaluate its activities. RED provides direction for the organization to get bigger and evolve. In 1977, BRAC shifted from community growth towards a more targeted approach by organizing village groups which is called Village Organizations. In 1979, BRAC entered the health field in a most important way. It established the nation-wide Oral Therapy Extension Program (OTEP), a campaign to fight diarrhoea, the leading cause of the high child mortality rate in Bangladesh. By ten years period 1,200 BRAC workers went doorto-door to coach 12 million mothers the preparation of home-made oral saline. Now Bangladesh has one of the highest rates of usage of oral rehydration. Oral rehydration therapy is a simple, cheap, and effective treatment for dehydration connected with diarrhea, particularly gastroenteritis, which is caused by cholera or rotavirus. BRAC’s campaign reduced child and infant mortality from 285 per thousand to 75 per 1000. In 1991 the Women’s Health Development program commenced (www.brac.net).
Case Study
Case Study -1 : Story of a BRAC SS
Mst. Mahima Begum (29), D/O- Late Ruhul Aamin & late Akasi Begum, Village-Puthia, Thana- Puthia, District Rajshahi, Bangladesh is working as SS from last four years. Her working area is Asulia of Savar. She shared her experience of BRAC’s activities. About 220 households are under her jurisdiction. Every day she visits 8-10 households by 2-3 hours. Her role and scope of performing social work as an SS, she is serving the pregnant and new mothers, children, TB patients and the common people of her locality, and thus helping her husband who is a rickshaw puller to maintain their family. She sits together with village women and asked them about their health issue. She distributes essential medicine at BRAC’s fixed rate. She collects sputum of suspected patients of TB, keep monitoring about existing TB patients DOTs course. She also distributes oral rehydration saline with BRAC’s fixed price for children and adults diahrroea patients. She also shared that, during her last four years, no diahrroea patient diet. The villagers are well known about oral rehydration saline.
People of that area like her for her cordiality and devotion to her work, and they are in tendency to come to her for solving their health related problems. And, she always tries her level best to provide them with all sorts of assist within her reach. Once some Mr Shamsu H/O-Segupta Begum came to her for informing that her wife’s labour pain had started, and she rushed there to help Shegupta to help her. But, the pain extended and time passed with no delivery. Then she informed the existing condition to the concerned SK and PO by mobile phone, and the PO given a motor vehicle for shifting the patient to the near Upazila Health Complex, where Shegupta gave birth to a male child under the supervision of the concerned medical officer. After some days, she came to know that some Shelly, W/O-Abdul karim encountered a serious problem of post-delivery bleeding, she went there immediately and made necessary measures for shifting her to the nearby UHC for superior treatment, and this mother also became safe. After this event she became more popular and her social acceptance increased a lot. She usually provides healthcare services for at least 10 common diseases among the people of her area, and they call her ‘Doctor Apa (A sister practicing as a doctor)’. Hearing about all her success story as an SS, the UM of BRAC Health Program, Savar one day to her house and wanted to make her the ‘Model Shebika’. It gave her huge satisfaction. The UM sent her for higher training meant for the ‘Model Shebika’, and after closing the training, when she came back to her operational area, her office gave her BP machine, Thermometer, Eye-chart, Pregnancy detecting Kit for using in her area to make sure better service delivery to poor. People from the locality come to her house for getting preliminary treatment of common diseases, for examination of eye-sight, BP-check, Pregnancy test, fever check and so on. She feels proud for being able to serve the common people. As a SS she is now well known to her community and she is happy to her job because she thinks that she is doing something for the community as well as for herself. She said about herself, “we, the uneducated women, perform a doctor’s job and give medicine to the villagers. This raises our status and honour. Even the moneyed people come to discuss with us.
I asked about SS to one village woman, and she said, “we regard her highly and talk about with her usually before going to a doctor; we know that she is not a doctor, but she can give explanation our problems. She is a general practitioner to us”.
I asked the SS about BRAC Health program’s effectiveness and causes of success. She told that, the continuous monitoring and suggestion from the BRAC’s SKs, POs and Ums are the prime factor of success. She receives every help she want from top supervisors as early as possible. So, she can help the community patients effectively.
Case Study-2: A DOTS TB patient
During the study, TB patients who are now taking medicine, have taken some their exclusive interview to know deeply about ongoing DOTS TB program. One of them is Md Masum whose story of TB is shared here to know details.
Md. Masum (42), Son of Md. Hakim, Present address Village: Khagan, Uninon: Birulia, Police
Station: Savar, District: Dhaka. He is a worker of Panna Textile Mill Ltd, Khagan. He told that he is working in Panna Textile since 17 years after his first arrival in Dhaka. He came from Kurigram District by the motivation of his uncle who was working Panna Textile. He said that he had a bad cough that lasts 3 weeks or longer with pain in the chest and coughing up blood in sputum. He met with a BRAC Health Worker (SS) and BRAC SS collect his sputum and sent it to Mohakhali National Institute of Chest Disease and Hospital. The report was negative and BRAC DOTS for TB took his treatment responsibility. He is now out of work as suggestion of SS and taking medicine regularly.
The medicine is free of cost because it is supplied by BRAC health division on behalf of government freely. He took medicine by going to SS home. If he failed to take medicine once, BRAC SS come to his home and asking about absent to take medicine, SS feed medicine. Now his health condition is better than before. Although he is now out of work, but he feels good because BRAC SS takes care of him regarding TB.
Case Study-3: A DOTS TB patient
Here is a case study of Ms Johra, who is also a TB patient taking medicine from BRAC health service.
Mosammmad Johra Khatun (26), daughter of Md Abul Hossain, Village Barihati, Uninon: Lalor, Police Station: Bera, District: Pabna. She is a worker of Blue Specific Jeans Wear Ltd, Jaleshwar, Savar bazar, Dhaka. She told that he is working in this garments since last 5 years. She lives with his co worker in Porabari, Savar where 6 persons lives in single room.
All together there are 37 workers in 7 tin shed. She said that he had a chest pain with bad cough with 25 days. Then she met with BRAC SS by the advice of her co workers. After testing sputum which is collected by BRAC SS, found that she is patient of TB. She feels very depressing after knowing that she is a patient of TB disease. Because she heard that TB is not curable disease. But after counseling with BRAC SS, she feels good and she is taking medicine regularly by going SS’s home. She also told that if she failed to go to the home of BRAC SS due to any reason, the BRAC SS come to her home and feed medicine. Now she is absent from his works. She feels better after taking medicine and she said that she cost nothing for the medicine and overall treatments, because BRAC is supplying medicine free of cost to them on behave of government. She is very much confident about her cure and she is grateful to BRAC for her caring in bad days and help to cure from TB disease.
Content analysis
Content Analysis 1: Data of diarrhoeal death comparison on 1980 and 2014 Bulletin of the World Health Organization (Volume 92, Number 9, September, 2014, 664-671) says that diarrhoeal death among aged 1 to 59 months is 2.8% for Bangladesh.
In the 1980s, five million children worldwide died every year because of diarrhoea, essentially because there was no readily available treatment. In the intervening 30 years, improved management of diarrhoea, such as treatment with oral rehydration solutions, intravenous fluids and zinc, has led to a substantial decrease in mortality to approximately 614 000 deaths every year. Nevertheless, diarrhoea remains a common cause of death in all children and is the second most common cause in those aged above 1 month (www.who.int)25.
The following Table shows the data of 2003-2008.
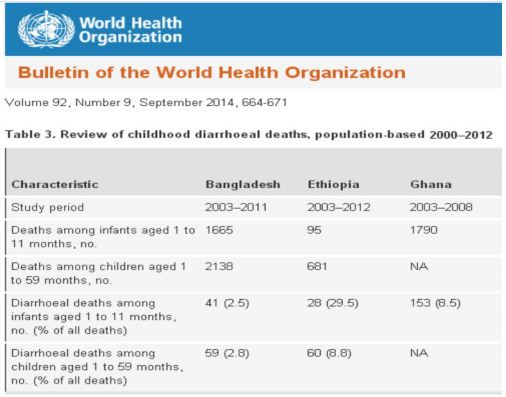
Table: Review of childhood diarrhoeal death
The Bangladesh Disease and Disease Control says at mid-1980s survey indicated that deaths due to diarrheal diseases, malnutrition, and pneumonia accounted for 16.3 percent, 13.1 percent, and 10.8 percent of all deaths, respectively(www.photius.com).
Learning from the above content:
This two data says that the rate of death due to diarrhoeal diseases is decreased from 16.3% in 1980 to 2.8% in 2012.
Content Analysis 2: An article of “globalpost” newspaper (The Italic font means the article is published here as is was in newspaper)
A simple solution: The history of ORS in Bangladesh DHAKA, Bangladesh: In the last 30 years, oral rehydration solution (ORS)- a blend of salt, sugar, and clean water – has saved an estimated 50 million lives worldwide, especially children at risk of contracting severely dehydrating, fatal diarrhea. In 1978 the British medical journal The Lancet called ORS potentially the most important medical advance of the 20th century. Diarrheal diseases are one of the world’s largest killers of children under age 5.
A simple electrolyte blend, ORS was formulated to treat cholera by US and Bengali researchers in the late 1960s at the Pakistan-SEATO, the predecessor to the International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B). The American researchers, a group of young doctors, had opted to go overseas as part of a US government program, in lieu of serving in the Vietnam War. At the time, the United States was more insular, and Third World diseases like diarrhea were not typically discussed in medical schools, said Dr. Richard Cash, one of the researchers.“You think I ever thought about diarrhea other than it messed up one of my vacations?” Cash said in a recent interview in Dhaka. “I was just in the right place at the right time.”
In the 1970s, BRAC (formerly Bangladesh Rural Advancement Committee), the wellknown Bangladeshi NGO, collaborated with ICDDR,B to devise a rigorously monitored process to teach mothers to make the mixture at home. Starting in 1980, more than 12 million Bangladeshi mothers were taught to make ORS, a program that saved countless lives, according to Cash’s book, “A Simple Solution.’
That knowledge took hold: Since 2007, the 2011 Bangladesh Demographic and Health Survey reports, about 78 percent of children with diarrhea have been treated with ORS, which is readily available at shops and clinics today. ORS is now a mainstream treatment around the world, with UNICEF distributing 500 million sachets to 60 countries each year.
Learning based on the above content:
A rigorously monitored process to teach mothers to make the mixture at home is important¸ Since 2007, the 2011, about 78 percent of Bangladeshi children with diarrhea have been treated with ORS¸ ORS is now a mainstream treatment around the world.
Content Analysis 3: Teaching ORT messages to millions: the BRAC case (The Italic font means the article is published here as is was in newspaper, source:
Basic conceptual issues of communication
Communication is a key instrument to bring change for development. It is a continual process to occur. People communicate with others aiming to modify their behavior towards better survival. Morton et al (1976) observed, “Communication reflects an attempt to influence another’s behaviour to produce physical, social or economic rewards.”
Communication is also used for making effective decision about what people think and what they do. Schramm (1964) said: Without adequate and effective communication, economic and social development will inevitably be retarded, and may be counterproductive. With adequate and effective communication, the pathways to change can be made easier and shorter. There are four types of communication in practice: (i) Intrapersonal, (ii) Interpersonal, (iii) Group, and (iv) Mass. All these directly or indirectly effect at intrapersonal level.
Different models of communication exist in the domain of communication. Of them, the Convergence Model and the Diffusion Model and/or the combination of both appear to be more effective for development communication. The Convergence Model is defined as a process in which the participants create and share information with one another to arrive at a mutual understanding (Rogers et al 1981). The Diffusion Model is concerned with the spread of messages.
Communication, indeed, is a tool for decision-making in partnership. The communicators facilitate the participants to make their own decisions. The participants can make skillful decisions when the communicators and the participants share facts and feelings.
Communicators and participants are, therefore, a vital partnership at the centre of communication. However, information about a specific subject reaches the people in many ways. In a good communication, the communicators and their participants frequently go through a series of interlinked and overlapping steps (Population Reports 1998). These steps can be remembered by the letters in the word “GATHER.” The word “GATHER” stands for:
G= Greet: Welcome each participant on arrival
A= Ask: Ask the participants for reason for coming, and encourage them to talk
T= Tell: Start discussion with the participants’ preference
H= Help: Help the participants to understand and let them decide
E= Explain: Provide what the participants want
R= Return: Plan the next visit, if needed
For a greater participation at the grassroots, the pattern and flow of the messages should be fashioned in a way that would help the grassroots to have easy access to knowledge and technology through their existing ordinary channels of communication in the rural community (Ouchi 1985). BRAC, one of the largest NGOs in the world, proved that even the illiterates could be empowered for development by communicating messages through appropriate culture sensitive channels. The following section documents the case of BRAC ORT teaching at household level.
BRAC’s oral therapy teaching program
BRAC has diversified approaches to communicate and sensitize the development participants about the overall development. The BRAC communication strategy can be
viewed at three levels viz; i) Grassroots level, ii) Training level, and iii) Organizational level (Arif 1996). As an organization BRAC generates information on development issues and needs by involving the people at various levels, and discusses these at policy level of the organization. Thus, interventions are designed and implemented. Since the BRAC management structure is flat, it is easy to communicate decisions to the concerned.
However, to implement the development programs the staff at all the tiers are given training at its training centres. Then, they begin work with the target people and get involved in continual communication at the grassroots. By using the interpersonal communication technique, BRAC successfully reached ORT messages to millions in Bangladesh. The reason for adopting this strategy among the many options was that most of the rural mothers were illiterate and superstitious. Therefore, to dispel wrong traditional beliefs and values of the learners, face-to-face teaching was instrumental and effective. BRAC’s approach was well acclaimed. In the ‘Foreword’ of the book titled “A simple solution: Teaching millions to treat diarrhoea at home” Jon E. Rohde wrote:
The story of the Oral Therapy Extension Program, OTEP is a tale of how a medical technology was adapted, revised and presented to an illiterate public through house-tohouse health education by a small army of dedicated health workers. Through a decade of persistent work, the entire BRAC organization initiated this ambitious program, and in spite of all skepticism from the global public health community, carried the science of oral therapy into every home in Bangladesh. Never before, or since, has a public health effort of this intensity been tried. Never before has health education been provided under such rigorous and cost-effective circumstances with constant monitoring, evaluation and resulting in improved implementation at progressively lower unit cost throughout the decade of the program.
Development of the BRAC ORT program
Oral Rehydration Therapy (ORT) has been a proven cost-effective tool for treating most types of diarrhoea. In the past, many developing countries implemented ORT program, some promoted packet oral rehydration solution (ORS) and others home solutions. As mentioned earlier, one of the biggest and widely acclaimed program was the one run by BRAC in the eighties in Bangladesh.
In the mid-seventies, BRAC promoted and distributed packet ORS through community volunteers and BRAC paraprofessionals. But the strategy envisaged many problems, particularly in terms of availability and distribution of the packets to the villagers, while cost and management were the other problems (BRAC 1980). BRAC then tried out an alternative. Field research revealed that a three-finger pinch of lobon (common table salt), and one scoop of gur (unrefined local sugar) in a half litre drinking water (467 ml) produced a solution having many needful properties of standard ORT. Lobon supplied sodium and chloride, while gur sucrose and some potassium. But the burning question was how to reach the technology to the doorstep of the rural people who need this most?
BRAC decided to experiment the process in its Sulla project. The pilot project sought answer to the following critical questions (for details, Chowdhury et al 1996):
- What would be the contents of the education messages? Research showed that for home management of diarrhoea BRAC should teach a mother/caretaker about diarrhoea and its effects, preparation and administration of solution with home ingredients, and dietary advice etc.
- Who would be taught the messages? Conventionally mothers are the caregivers to the children and other family members. Therefore, they were the prime targets for ORT education. While the adolescent girls are would-be mothers, they were also targeted for the same.
- How would the messages be taught? Many options were considered such as radio, village level meeting of the mothers, and one-to-one teaching. Since a very few mothers had access to radio, and it was not culturally feasible to assemble the mothers in a common place of a village, the third option i.e., individual teaching approach was adopted.
- Who would teach? Since rural women were the targeted learners, the women were made primary workers for teaching.
Through this trial BRAC also developed a “Seven Points to Remember” which contained a concise but comprehensive messages on the definition of diarrhoea, cause of diarrhoea, preparation and administration of ORT, nutritional advice etc. Mothers could easily remember these messages and prepared safe ORT when taught. The locally trained females Oral Rehydration Workers (ORW) with 8-10 years of schooling were capable to teach the mothers.
From July 1980 through December 1990, BRAC health workers visited about 13 million rural households to teach the rural mothers about the BRAC innovated ORT popularly known as lobon-gur saline (LGS).
Operational methods
House-to-house teaching: One woman from each household was taught the core of the “Seven Points to Remember” at home. For this, the ORWs used to travel from temporary residences on foot or by rickshaw or country boat based on the local communication system and season. While visiting home an ORW was to introduce herself to the woman first and engaged in a friendly chat. Thus, she gradually moved to the conversation on the “Seven Points to Remember.” The ORW ensured two-way communication and invited queries from the woman, and thereby clarified, if any. During the teaching session, the ORW also demonstrated how to measure water (half litre) in a household container and put a mark inside the container so that the woman could measure a half litre water accurately. Then the woman was asked to prepare LGS herself. Lastly, the ORW used to review main points of the session to make sure that the woman fully understood the “Seven Points.” During teaching, the ORW used a flip chart containing pictorial illustrations of all the points. At the end of each session, the ORW used to record the village, the para (cluster of household), the woman’s name and the name of the household head in her diary given by BRAC. This helped identify the woman for post-education follow-up. Each home visit took 30-35 minutes enabling an ORW to cover 8-10 households a day.
By 1986, about one-third of the rural households was taught through one-to-one teaching method. This helped develop a congenial atmosphere towards female workers’ mobility in the villages since news of the program reached many opinion leaders in the uncovered areas. At this stage, the mode of teaching was changed and instead of one-to-one teaching at a time, the ORWs started group teaching. The approach created an interactive environment among the participating women for quick learning. Even the learners in the session helped each other to learn. Moreover, the teaching cost reduced by half without affecting the quality of the program (Chowdhury et al1988). An ORW then taught about 20 women a day.
Quality control: A two-tier mechanism was in place for quality control, viz, i) ongoing monitoring system, and ii) operations research and evaluation.
Monitoring: There was an in-built monitoring system run by the program itself by involving separate monitor teams. The Area Managers directly supervised these teams.
The monitors visited five to ten per cent of the households, already taught by the ORWs at least one month earlier, to assess the core issues of ORT teaching:
- a) how well they taught women remembered the Seven Points,
- b) the skill and accuracy of these women in preparing the LGS, and
- c) use of LGS in diarrhoea episodes in the last two weeks.
The monitor collected a small sample of solution in a crew-cap vial. The samples were analyzed for chloride concentrations in the field laboratories and ten per cent of them (as analyzed in field lab) was analyzed for sodium, potassium and glucose at the laboratory of the International Centre for Diarrhoeal Research, Bangladesh (ICDDR,B). Each woman monitored was graded according to her answer on the Seven Points on a score of ten and her ability to prepare a correct solution. The women, who could remember all the Seven Points and prepare correct LGS, were given A grade; grade B means that an woman scored 7-9 points and prepared the LGS correctly; grade C means that she scored less than 7 points but still could prepare the LGS correctly; and grade D means that she failed to make correct LGS. Based on this grading, the ORWs received incentive salary (Taka 4 for each visited household in grade A, Taka 2 in grade B, Taka 1 in grade C, and none in grade D). This means that an ORW did not get remuneration if the mothers she taught failed to make the LGS correctly. The main purpose of such incentive salary system was to ensure the quality of the teaching program.
Operations research and evaluation: The Research and Evaluation Division (RED), an independent wing within the BRAC, continuously conducted a number of studies to improve the program quality to a further extent. Many research findings were used in program development. For instance, male contact was introduced to win the support of the male, efforts were made to dispel doubts about ORWs’ intentions, Seven Points were revised to accommodate people’s perception on diarrhoea and group teaching was introduced.
Male contact: Males play a predominant role in family decision-making. So unless they are convinced it would be difficult to popularise the ORT. In the early days of the program the males were not taken into confidence. Therefore, BRAC later used a number of fora to win the support of the males.
Village doctor meeting: Huge numbers of village doctors involved in healing practice are very popular to the villagers. To develop their positive attitude towards LGS, BRAC workers arranged meetings with them to disseminate the ORT messages.
School meeting: BRAC organized meetings in primary and high schools, and madrashas and taught Seven Points to the teachers and students. Most of them became active promoters of ORT in their own homes.
Mosque meeting: Each village has a mosque led by clergies who have influence in moldings people’s opinion. BRAC arranged meeting on Friday congregations and got the people convinced by the clergies so that they use LGS in diarrhoea.
Village bazaar: The BRAC workers organized meetings in different haats/bazaars where people assembled for shopping.
Patient demonstration meeting: During teaching ORT at household level, the ORWs and Program Organizers used to search for diarrhoeal cases and treat them with LGS. The POs used to follow up the cases on the following day. They organized meeting in the respective villages along with the cured patients. This directly helped develop people’s confidence on the efficacy of LGS leading to an increased usage.
Other fora: The male workers contacted the people individually wherever possible. Print materials: BRAC also developed and produced a variety of print materials, which included posters, leaflets, and flip charts. The latter one was used by the ORWs in teaching sessions while the others were distributed in villages.
Billboard: BRAC installed billboards with core messages on ORT in suitable locations of the country.
Radio and TV: BRAC aired a number of messages on diarrhoea and its home management through radio and TV. The most important benefit of this drive was that it gave credibility to what the ORWs and other workers had been trying to tell the villagers through house-to-house visits.
Influencing policy: The Bangladesh government has its own program on ORS packet promotion, which was to mix in one litre of water. But BRAC one was to mix in a half litre of water. However, to make it uniform the government accepted the standard of half litre for Bangladesh and produced half-a-litre packets. All the commercial producers also followed the standard.
Training: All the workers were properly trained before being sent to the field. Besides, refresher training were organized quarterly.
Reinforcement: The ORWs taught the mothers following the ‘reach, teach and leave’ method. Later BRAC introduced reinforcement teams who repeated the ORT messages while visiting villages for imparting education on immunization and vitamin A.
Supervision: A team coordinator, who was one of the two male members of the ORW team, was responsible for primary supervision. He was accountable to the Area Manager. The Program Manager from the Headquarters oversaw the whole program with the help of Regional Managers.
Some results
Coverage: The program visited about 13 million rural households out of approximately
15million.
Knowledge retention: Study carried out in 1993 (Chowdhury et al 1997) revealed that over 70% of the mothers could prepare a chemically ‘safe and effective’ ORS. A significant number of these others were very young at the time of the mass campaigns using house-to-house teaching, plying an intergenerational transfer of the knowledge on ORT.
Use of ORT in diarrhoea: Any form of ORT use rate in all types of diarrhoeal episodes was more than 50%. When considered the severe or watery diarrhoea about 83% episodes were treated by ORT (Chowdhury et al 1997).
Learning from the above content:
It is very successful to spread messages to the grassroots citizens through interpersonal communication.
- In-house research is positive for program development. Mothers, irrespective of their literacy, have the capacity to learn improvement information.
- Flexibility in plan and execution improves program’s effectiveness. Such a condition helps redefining the program goal and strategies as and when essential.
- People’s sharing in developing messages vis-a-vis methods of communication can play a significant role in program’s achievement.
- NGOs can execute countrywide program.
- Monitoring and follow-up are vital for a successful communicative program.
Conclusion
Conclusion
BRAC has adopted an experimentation-expansion evaluation model to build up and deliver it’s the programs. Lessons learned from own experiences in public health, like the bare-foot doctors of the 1970s, Oral Therapy Extension and Child Survival programs in 1980s,Women’s Health, Reproductive Health and Disease Control programs in 1990s, have enabled BRAC to expand sustainable and accessible health care to more that 100 million people across Bangladesh (www.brac.net). BRAC also collaborate on national projects for instance Vitamin-A supplementation and family planning initiatives. By choosing health volunteers, or Shasthya Shebikas, from BRAC’s own Village Organizations (VOs), BRAC is making efficient use of resource and is able to make sure sustainability unlike other programs in the health sector. SS and SK, who attempt to address the crisis of human resources in the health division by playing an significant role in providing accessible and reasonable services to the majority of the population. SS receives basic training and provides door-to-door health education, treat basic illness, refer patients to health centers and provide necessary health items and medicines; which contribute towards an earnings for the volunteer.
Essential Health Care (EHC) has evolved to be BRAC’s central part health intervention where BRAC CHWs offer low cost essential health care services to over 100 million people across the country with a special emphasis on very poor families. BRAC have started maternal, neonatal and child health (MNCH) programs. A referral system is developed which facilitates transfer of acute emergency cases to hospitals. The contribution of SS in detecting suspected TB cases, collecting sputum for lab diagnosis and ensuring community based directly observed treatment short courses (DOTS) for TB is tremendous. BRACs collaborative efforts reach all the 13 malaria risk prone districts, accounting for direct service provision in four districts. The CHWs identify malaria symptoms, conduct blood tests using the rapid diagnostic test and provide treatment at the community level. For addressing malnutrition, BHP has started to implement the community component of Alive & Thrive. BHP has reached well over 12 million people in 50 sub districts to reduce stunting by promoting exclusive breast feeding and complementary feeding. In an attempt to prevent and control anemia of under five children, BRAC distribute Sprinkles for ensuring intake of iron and other essential elements with the support of BRAC’s CHWs in 61 districts. Aligned with the government’s commitment to Vision 2020, BRAC are implementing Vision Bangladesh, which reduces the backlog of cataract blindness by carrying out surgeries in Sylhet. In addition, to correct presbyopia (faulty near vision), BRAC screen people above 35 years and supply them with reading glasses through Shasthya Shebikas in 24 districts. Through collaborative eye care projects, BHP strives to avert preventable eye problems.
From the above study, learning from BRAC health innovations are:
- BRAC found a local woman in each village area and trained her on all of the familiar diseases that could be found in the area can keep character in as trained nurses.
- Careful selection, training, encouraging supervision, functional recommendation relation and performance-based encouragements are key factors responsible for the sustenance of Community Health Worker or Shyasta Shebika.
- Oral Rehydration Saline was invented by ICDDRB, Dhaka and BRAC has promoted the home-made ORT solution for apply in all diarrhoeal episodes called lobon-gur solution (LGS) using the ‘pinch-and-scoop’ process, made by mother in her home, can save a child life.
- Prevention of diseases such as measles, poliomyelitis, and diphtheria concurrent with widespread use of ORS for diarrheal diseases has considerably decreased childhood mortality and morbidity.
- From organizing mobile outreach to collect sputum samples for diagnosis to implementing a bonding system to make sure treatment compliance, BRAC’s shows how programmatic innovation and sound managing systems can enable an organization to attain some of the highest cure rates (94%) while operating at unprecedented scale.
- To understand that it is vital to carry on learning from the experiences achieved by an approach, by the failures as well as the successes, and to find a means to go forward continuously.
- The leadership of BRAC is totally innovative. It confident new approaches while constantly asking for proof of together impact and sustainability. Based on the on a daily basis meetings which took place each evening to share the experiences of the day, and the community gatherings in which plans and progress were discussed, BRAC critically examined and then documented its experiences in close collaboration with those it served.
- With the active engagement of community health workers and birth attendants BRAC have demonstrated that with limited resources, it is possible to change behavior and practices to lower the incidences of maternal and neonatal deaths within a short period.
- BRAC has managed the demand and supply chain and ensuring excellence of health sector.
- Fund-raising became a matter of recording and disseminating the lessons of development, when success brings success.
- Working in collaborative with the government and different NGOs in combating TB and malaria makes a successful example of public private partnerships.
- BRAC’s healthcare programs is the example of low cost and simple know-how integrated within a development context could produce similar results in comparison to high cost, sophisticated intensive methods
- A awareness of the changing health needs, adjustment of technology, cost effectiveness, sustainability and delivery through partnerships with communities and government are key features in BRAC’s approach to providing healthcare to poor people.
- The health impact of BRAC is closely related to its approach: its partnership with those it serve, its respect for women, particularly poor women, its attention to effective support, management and evaluation, and above all, its inspiring leadership. BRAC’s personnel and their partners believe that a better life is possible for all, and by their actions plan to realize this belief.
- Through recognizing the multidimensional nature of poverty, BRAC seeks a holistic approach to its programs. The comprehensiveness of programs acknowledges that improving the health of the people of Bangladesh cannot occur without development in all essential areas including education, economic, and social spheres in a strategic approach to counteract poverty through livelihood generation and sustainability.
Further Scope of Studies
In fact, BRAC Health Innovations are the success stories in only for BRAC Health Programs. BRAC has several programs in education, microfinance, commercial sectors in different countries in world. Each program has some specific innovations, strategy and approach to bring it success. As BRAC is now world biggest NGO, so all programs of BRAC’s innovations and strategies are important to share with other organizations. Like BRAC, others successful NGOs in world may have some specific approach to make those fruitful. But due to time constraints the researcher could not address all the NGOs health innovations and other programs innovation stories. So, there is a greater scope for the future researchers to work BRAC health innovations as well as other NGOs health innovations and others NGOs programs success stories to share those all to build a sustainable developed world all together.