The main objective of this presentation is to analysis Carcinoma Gallbladder and Management. Other objectives of this Presentations are to observe the pattern of clinical presentation of carcinoma gallbladder, to determine the age and sex related incidence of carcinoma gallbladder and to observe the management according their presentation. Finally this report make swot analysis Carcinoma Gallbladder and Management.
INTRODUCTION
Carcinoma of the gallbladder (CaGB) is the most common malignant lesion of the biliary tract and holds fifth place among all malignant neoplasms of the digestive tract. It (CaGB) is a highly lethal disease. In over 70-80% cases, it is associated with cholelithiasis, although a correlation between these two cannot be determined with certainty.1 Even today, with multiple diagnostic tests available, gallbladder cancer is usually first recognized during a laparotomy performed for presumptive diagnosis of benign gallbladder disease. One to two percent patients undergoing operations for cholelithiasis have the diagnosis made incidentally at the time of surgical exploration.2 In India, however, the majority are discovered with advanced disease during ultrasonography for upper abdominal symptoms. In our country, the picture is almost same.
The incidence of gallbladder cancer varies greatly in different areas of the world. Highest incidence rates are seen in American Indians, people of Chile and other Latin American countries, Poland and North India. Though the incidence of carcinoma gallbladder in our country is no less than the western world, there is no broad-based study regarding this. So the exact incidence of carcinoma gallbladder in our country is not evaluated till now. But it is highly important to carry out a proper large scale study of these cancers in our country. Because the knowledge about the incidence, clinical presentations, evaluation of different patterns of treatment and natural history of the disease will invariably strengthen our efforts to combat the killer disease. Though it is not an uncommon disease in our country, there is dearth of information regarding this disease in this region. Pattern of presentation may also vary from other studies. By doing this, at least, awareness may be developed among the general people as well as the clinicians. For all these reasons, this has been chosen the topic of my study.
This study: “Different Pattern of Presentation of carcinoma gallbladder and management” done in BSMMU, Dhaka during the period of September, 2008 to August, 2009. In preparing the study, all possible efforts were made at finding, the incidence, clinical presentations, pathological correlations and treatment. I have tried my best to study these case thoroughly with special emphasis to clinical patterns of presentation and pathological corroboration. The operative findings, procedures applicable to the various cases and post operative clinical course were also studies but, of course, with some limitations.
ANATOMY OF THE GALL BLADDER
Embryology of the gall bladder and biliary tree
The liver primordium appears in the middle of the third week as an outgrowth of the endodermal epitheliurn at the distal end of the foregut. This outgrowth, the hepatic diverticulum, or liver bud, consists of rapidly proliferating cells that penetrate the septum transversum, that is, the mesodermal plate between the pericardial cavity and the stalk of the yolk sac. While hepatic cells continue to penetrate the septum, the connection between the hepatic diverticulum and the foregut narrows, forming the bile duct. A small ventral outgrowth is formed by the bile duct and this outgrowth gives rise to the gall bladder and the cystic duct. Liver cords differentiate into the parenchyma and form the lining of the biliary ducts.3
Gross anatomy of the gall bladder and biliary ducts
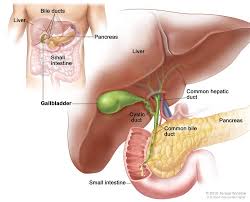
The hepatic ductal apparatus consists of intrahepatic and cxtrahepatic bile ducts. The extrahepatic ducts consist of
- The common hepatic duct, formed by the junction of the right and left hepatic ducts.
- The gall bladder, a reservoir of bile.
- The cystic duct of the gall bladder.
- The bile duct, formed by the junction of the common hepatic and cystic ducts.
The common hepatic duct
The main right and left hepatic duct issued from the liver and unites near the right end of the porta hepatis as the common hepatic duct, which descends about 3 cm before being joined on its right at an acute angle by the cystic duct to form the main bile duct. The common hepatic duct lies to the right of the hepatic artery and anterior to portal vein.
The gall bladder
The gall bladder is a slate blue, piriform sac partly sunk in a fossa in the right hepatic lobe’s inferior surface. It extends forwards from a point near the right end of the porta hepatis to the inferior hepatic border. It is 7-10 cm long, 3 cm broad at its widest and 30-50 ml in capacity. It is described as having a fundus, body and neck. The fundus, the expanded end, projects down, forwards and to the right, extending beyond the inferior border to contact the anterior abdominal wall behind the 9th costal cartilage. The body is directed up, back and to the left; near the right end of the porta it is continuous with the gall bladder neck. The neck (cervix) is narrow, curving up and forwards and then abruptly back and downwards, to become the cystic duct, at which transition there is a constriction. The neck is attached to the liver by loose connective tissue containing the cystic artery. The neck also shows a dilatation; the infundibulum (Hartmann’s pouch), which hangs downwards and is often connected to the duodenum by folds, which may be either congenital or inflammatory in origin.
The cystic duct
This structure is 3-4 cm long; it passes back, down and to the left from the neck of the gall bladder, joining the common hepatic duct to form the bile duct. Its mucosa forms spiral valve5.
The bile duct
The bile duct is formed near the porta hepatis, by the junction of the cystic duct and common hepatic duct; it is usually about 7.5 cm long and 6 mm in diameter.
It is divided into four parts:
- The supraduodenal portion, about 2.5 cm long, running in the free edge of lesser omentum.
- The retroduodenal portion.
- The infraduodenal portion lies in a groove but at times in a tunnel, on the posterior surface of the pancreas.
- The intraduodenal portion passes obliquely through the wall of the second part of the duodenum where it is surrounded by the sphincter of Oddi. It terminates by opening on the summit of the ampulla of Vater.
Left of the descending part of the duodenum the bile duct reaches the pancreatic duct; together they enter the duodenal wall where they usually unite to form the hepatopancreatic ampulla, which opens on the summit of the major duodenal papilla
MICROSCOPIC STRUCTURE OF THE GALL BLADDER AND BILIARY DUCTS
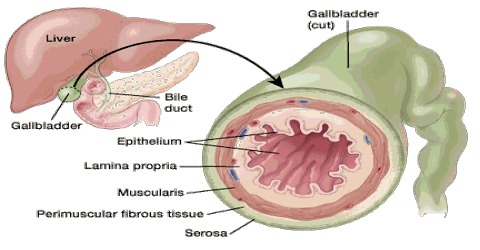
- The wall of the gall bladder displays three layers. The layers are: Serous, fibromuscular and mucous.
- The serosa completely covers the fundus but only coats the inferior surfaces and sides of the body and neck of the gall bladder.
- The fibromuscular layer is composed of fibrous tissue mixed with smooth muscle cells arranged loosely in longitudinal. circular and oblique bundle.
- The mucosa is loosely connected with the fibrous layer, is generally yellowish brown and elevated into minute rugae with a honeycomb appearance.
Its epithelium is a single layer of columnar cells. The mucous membrane contains indentations of the mucosa that sink into the muscle coat; these are the crypts of Luschka. There is no gland in the mucosa but mucus is secreted by the epithelium itself. The basal intercellular spaces show considerable dilatation and many capillaries lie close to the basement membrane. These features indicate active absorption of water and solutes from the bile, rendering it more concentrated. Mucous granules are present in the apical half of some cells, particularly those near the duct; these are secreted into the lumen.
The coats of the large biliary ducts arc an external of fibrous layer. The fibrous layer is composed of fibroareolar tissue; intermingled with a few non-striated muscle fibre that are arranged in a longitudinal, oblique and circular manner. The mucous layer is continuous with the lining membrane of the hepatic ducts and gall bladder and also with that of the duodenum. Its epithelium is of columnar variety.
Many lobulated mucous glands are present. In the bile ducts, the mucous membrane is provided with numerous tubulo-alveolar glands that secrete mucin.
The circular muscle around the lower part of the bile duct, including the ampulla and the terminal part of the main pancreatic duct, is thickened and is called the sphincter of the hepatopancreatic ampulla (or the sphincter of Oddi). The later comprises musculature at three levels:
(i) at the end of the bile duct (sphincter ductus choledochus);
(ii) around the terminal part of the pancreatic duct (sphincter ductus pancreatici); and
(iii) around the ampulla.
Only the choledochal sphincter is constantly present 5.
Blood supply
Arterial supply
The cystic artery, usually from the right branch of the hepatic artery proper, it passes behind the common hepatic and over the cystic duct to the superior aspect of the gall bladder’s neck, on which it descends to divide in to superficial and deep branches. The former ramifies on the inferior, the latter on the superior aspect. An accessory cystic artery may arise from the common hepatic or one of its branches. The cystic artery supplies the hepatic ducts and upper part of the common bile duct. The lower part of the bile duct receives rami from the cystic artery. The right hepatic artery supply intermediate part through very small rami, the main supply being from the cystic and posterior superior pancreaticoduodenal arteries.
Venous drainage
The cystic veins, which drain the gall bladder, vary. Those from its superior surface are in areolar tissue between the gall bladder and liver, usually entering the liver through the visceral fossa to join the hepatic veins. The remainder form one or two cystic veins which commonly also enter the liver either directly or after joining the veins draining the hepatic ducts and upper bile duct. Only rarely does a single or double cystic vein drain into the right portal branch.
Lymphatic drainage of the gall bladder and bile ducts
Numerous vessels run from the submucosal and subserosal plexuses on all aspects of the gall bladder and cystic duct, those on the former hepatic aspect connecting sparsely with the hepatic vessels. They pass to the hepatic nodes, especially the cystic nodes and node of the anterior epiploic border. Hepatic nodes also collect from vessels accompanying the hepatic ducts and the upper part of the bile duct, those of its lower part draining into the inferior hepatic and upper pancreaticosplenic nodes. Subserosal lymphatic vessels of the gall bladder also connect with the subcapsular lymph channels of the liver, and this accounts for the frequent spread of carcinoma of the gall bladder to the liver.
Nerve supply
Sympathetic and parasympathetic innervation is from the coeliac plexus exist in the muscular and submucosal layers pass along the hepatic artery and its branches. Fibres from the right phrenic nerve, through communications between the phrenic and coelic plexuses, appear to reach the gall bladder via hepatic plexus, thus explaining the referred “shoulder pain” in gall bladder pathology. Sympathetic nerves are motor to the musculature of the gall bladder and bile ducts, but inhibitory to the sphincters of the bile duct. Gall bladder pain via vagus is referred to the stomach.
PHYSIOLOGY OF THE GALL BLADDER
Functions of the gall bladder
- The gall bladder is a reservoir for bile. During fasting resistance to flow through the sphincter is high, and bile excreted by the liver is diverted to the gall bladder. After feeding the resistance to flow through the sphincter of Oddi is reduced, the gall bladder contracts and the bile enters the duodenum. These motor responses are in part effected by the hormone cholecystokinin.
- Concentration of bile by active absorption of water, sodium chloride and bicarbonate by the mucous membrane of the gall bladder. The hepatic bile, which enters the gall bladder, becomes concentrated 5-10 times.
- Secretion of mucous — approximately 20 ml is produced per day.
Physiology of bile
Bile is made up of the bile salts, bile pigments and other substances dissolved in an alkaline electrolyte solution that resembles pancreatic juice. About 500 ml is secreted per day. Some of the components of bile are reabsorbed in the intestine and excreted again by the liver (enterohepatic circulation)
The glucuronides of the bile pigments, bilirubin and biliverdin are responsible for the golden yellow colour of the bile. The bile salts are sodium and potassium salts of bile acids, and all those secreted into the bile are conjugated to glycine or taurine.
Storage of bile in the gall bladder
The bile secreted continually by the liver cells is normally stored in the gall bladder until needed in the duodenum. The maximum volume of the gall bladder is only 30-60 milliliters. Water, sodium chloride and most other small electrolytes are continually absorbed through the gall bladder mucosa, concentrating the other bile constituents, including bile salts, cholesterol, lecithin and bilirubin. Bile is normally concentrated about 5- fold, but it can be concentrated up to a maximum of 20-fold.
By far the most potent stimulus for causing the gall bladder contractions is the hormone cholecystokinin. However in addition to cholecystokinin, the gall bladder is also stimulated less strongly by cholinergic nerve fibres from both the vagi and the enteric nervous system.
Pathology
Carcinoma of the gallbladder usually produces diffuse thickening of the gallbladder wall with infiltration to surrounding structure. Most often these cancers originate in the gallbladder fundus. As the tumour progresses the gallbladder may fill with tumour and may contain purulent material, mucus or stones. Early carcinomas may appear as a mucosal plaque, a polypoid or papillary excrescence or discrete thickening of the wall. Macroscopically carcinoma gallbladder(CaGB) can be divided into papillary, tubular and nodular forms (Sumiyoshi et al 1991). Papillary tumours are less likely to directly invade the liver and have lower incidence of lymph node metastases.
There arc several histopathological types of CaGB. The majority of CaGB are adenocarcinomas (80-95%), which can be papillary, tubular, mucinous or signet cell type. The other histopathological types decreasing order of frequency are undifferentiated or anap1astic carcinoma (2-7%), squamous cell carcinoma (1-6%) and adenosquamous carcinoma (1-4%) (Henson et al 1992, Alborcs-Saavedra et al 1992, Misra et al 1995). Rare malignant lesions are carcinoid tumours, malignant melanomas, lymphomas and sarcomas.
Knowledge of the mode of spread of CaGB is important for developing a rational therapeutic approach to surgical resection. Fahim and colleagues (1962) emphasized the following modes of spread of CaGB- direct. lymphatic, vascular, neural, intraperitoneal and intraductal. The lymph from the gallbladder drains by lymphatic plexuses to lymph nodes along the biliary ductal system— the first level lymph nodes subsequently it spreads to the superior, anterior and posterior pancreaticoduodenal lymph nodes- the second level of lymph nodes. Further drainage is to coeliac. superior mesenteric and para aortic lymph nodes- the third level of lymph nodes. The lymph nodes at the hilum of the liver are affected by metastases in a retrograde fashion only. About 25% of patients with CaGB will have node metastasis at the time of operation or autopsy (Beltz and Condon, 1974).
Venous blood from the gallbladder drains into segment IV of the liver by short, direct, communicating veins or by accompanying the extra hepatic ducts into the liver. This drainage explains the initial localized metastasis of gallbladder cancers into the liver adjacent to the gallbladder rather than to distant sites in the liver. Fahim and associates (1962) demonstrated microscopic vein invasion in 13.9% of their cases. According to Ouchi et al, 66% of gallbladder veins end in the intrahepatic portal branches of the right lobe, 6% exclusively in the left lobe and 28% in both. Therefore, removal of a portion of liver is recommended as part of treatment for CaGB. Direct invasion of tumour into adjacent liver segments IV and V and other surrounding organs such as duodenum, colon, anterior abdominal wall and common hepatic ducts are the commonest mode of spread. Intraperitoneal dissemination from CaGB is uncommon. Intraductal spread is seen in 19% of papillary carcinomas. Perineural spread occurs in 24% of cases.
Staging
Several systems exist. Although a TNM system for staging biliary cancer has been adopted recently, the staging system developed by Nevin et al (1976) has been used widely. This system is based on the level of tumour invasion and correlated well with prognosis.
A simplified version of the American Joint Commission on Cancer (AJCC) staging is seen in Table 2.1 in the following section.
Table: American Joint Commission on Cancer Staging
| TNM* Definition | Tumor Location |
| Tis | Carcinoma in situ |
| T1a | GB wall: mucosa |
| T1b | GB wall: Muscle |
| T2 | Perimuscular connective tissue |
| T3 | Serosa or one organ, Liver <2 cm |
| T4 | Two or more organs, liver > 2 cm |
| N1a | Hepatoduodenal ligament nodes |
| MO | No distant metastases |
| M1 | Distant metastases |
* Tumor, node, metastases (TNM) staging classification
Table: Staging of Cancer of the Gallbladder
| Stage 0 | Tis | N0 | M0 |
| Stage 1 | T1 | N0 | M0 |
| Stage II | T2 | N0 | M0 |
| Stage III | T1-2 T3 | N1 N0-1 | M0 M0 |
| Stage IVA | T4 | No-1 | M0 |
| Stage IVB | T1-4 T1-4 | N2 N0-2 | M0 M1 |
The Nevin-Moran staging system is more commonly used and is seen in Table
Table: Nevin-Moran Staging
| Stage | Tumor Location |
| I | Intramucosal Cancer |
| II | Mucosa and muscularis involved |
| III | All 3 layers involved |
| IV | All 3 layers and cystic duct lymph nodes involved |
| V | Liver or distant metastases involved |
CLINICAL PRESENTATION
Early CaGB is not associated with specific symptoms and signs, but nonspecific symptoms have been grouped into five clinical syndromes (Piehier & Crichiow 1978), which are given below in decreasing order of frequency.
- Acute cholecystitis — some patients with symptoms suggesting acute cholecystitis. About l% patients operated on for acute cholecystitis have CaGB. Patients with this acute cholecystitis syndrome have an earlier stage of carcinoma with an improved survival rate.
- Chronic cholecystitis — these patients with occasional vague right hypochondriac pain with non-specific symptoms like nausea, vomiting and anorexia.
- Biliary tract disease — these patients exhibit symptoms of jaundice, weight loss, generalized weakness and right upper quadrant pain. Patients with this clinical syndrome have extensive disease.
- Clinical features of malignancy outside the biliary tract- anorexia, weight loss, generalized weakness and local complications of the tumour, such as fistula or invasion of adjacent organs. These patients usually have extensive disease.
- Benign manifestations outside the biliary tract — this small group of patients presents with gastrointestinal bleeding and upper gastrointestinal obstruction. Jaundice is frequent, and is an ominous finding. It was associated with unresectable disease in approximately 14% of our patients (Misra et al 1995).
Patients with advanced disease may also present with a palpable gallbladder mass, hard nodular liver and malignant ascites from carcinomatosis.
In 15-20% of patients, CaGB is discovered incidentally at the time of routine cholecystectomy or postoperatively on histology. Only 20% of patients have disease confined to the gallbladder at the time of diagnosis. The majority (80%) have locoregionally advanced disease with invasion of adjacent organs or, less commonly, distant metastases (stage III and IV) at the time of presentation. CaGB may be suspected in patients with a long history of chronic cholecystitis with cholelithiasis in whom a recent change in symptomatology and pain has occurred.
Investigations
Ultrasonography
It is now clear that early CaGB may be detected by ultrasonography (USG). Early tumours can be recognized by the presence of a polypoid mass projecting into the lumen (fixed and not associated with acoustic shadowing), complex mass filling the lumen and localized thickening of gallbladder wall. However, differentiation from cholecystitis poses some difficulty because thickening of the gallbladder wall can be seen in both diseases.
Advanced tumours, in addition, show loss of interface between gallbladder and liver, indication of tumour invasion, lymph node and hepatic metastasis, dilated bile ducts and ascites. USG can also identify polyps and demonstrate the presence of associated gallstones. The diagnostic accuracy of USG is over 8O%. Recently, with the advent of colour Doppler ultrasonography, one can differentiate between biliary sludge and carcinoma by seeing fine vessel pattern. Endoscopic ultrasonography (EUS) has also been used for diagnostic evaluation and it predicts the depth of tumour involvement with accuracy.
Computed tomography
Computed tomography (CT) accurately demonstrates gallbladder abnormalities and extent of disease. The diagnostic accuracy of CT is 60% and is lower than that of ultrasonography.36 The common CT findings in CaGB are a mass, almost filling the gallbladder lumen, or a polypoidal mass protruding into the lumen or an infiltrating tumour to liver seen as a focal or diffuse thickening of the gallbladder wall. The frequent finding is the presence of mass in the gallbladder fossa, with the gallbladder itself being indiscernible (Kumar and Aggarwal, 1994). Newer scanners of Spiral CT provide biliary and vascular reconstruction. It is also helpful in monitoring response to treatment. Computed tomographic angio-portography (CTAP) is useful in evaluation of hepatic metastases.
The main purpose of performing CT is to diagnose tumour extent- direct infiltration in adjacent tissue or vessels, lymph node and distant metastases. It has proved extremely useful in patients with advanced disease in deciding about surgery and the extent of resection required.
Magnetic resonance imaging
Only limited experience exists on the use of magnetic resonance imaging (MRI) in the evaluation of CaGB. The morphologic appearances of CaGB are similar on MRI and CT. the tumour appears hypointense on T1 weighted images and hyperintense on T2 weighted images. It is especially useful in visualizing tumour invasion into the hepatoduodenal ligament, portal vein encasement and lymph node involvement. No large series have compared CT and MRI37 Magnetic Resonance Cholangiopancreatography (MRCP) can evaluate malignant biliarv stricture (hilar cholangiocarcinoma) avoiding the complications of ERCP.
Selective angiography
Selective angiography has a high degree of diagnostic accuracy because it may show encasement of vessels of neovascularisation suggesting the diagnosis. Angiography is rarely used for diagnostic purpose, but it is of some value in assessing tumour extension and providing information regarding the resectability of the tumour.
Cholangiography
Cholangiography [intravenous cholangiography, endoscopic retrograde cholangiopancreaticography (ERCP) and percutaneous transhepatic cholangiography (PTC)] is of little value in detecting the presence of CaGB, because the gallbladder is not visualized in most cases. however. direct cholangiography such as ERCP and PTC arc helpful in planning operative procedures since they can demonstrate tumour growth in adjacent intrahepatic ducts,38 or in the common bile duct, ERCP is particularly useful when cholangiography is required in the absence of dilated intrahepatic biliary ducts.
Hepatoiminodiacetic acid scan (HIDA Scan)
A HIDA scan reveals only non—visualization of the gallbladder, which may be due to acute cholecystitis or, rarely, CaGB obstructing the cystic duct.
Ultrasound or CT guided fine needle aspiration cytology
Ultrasound or CT guided fine needle aspiration cytology (FNAC) for preoperative cytodiagnosis has been with increasing frequency. Reported sensitivity is 88%.39 This technique has particular relevance for proving the diagnosis in suspected cases of CaGB and in advanced cases where non-operative treatment of CaGB is being planned. Brushings of the obstructed bile ducts or bile cytology studies have a low diagnostic yield.
Laparoscopy and biopsy
Laparoscopy and biopsy are extremely useful in assessing peritoneal metastases, extent of disease and operability in patients with locally advanced disease.
Positron Emission Tomography (PET)
It is useful in detecting recurrent malignancy, particularly detection of small volume disease. It is also helpful in monitoring response to treatment. Although there is a difficulty in distinguishing between inflammation and tumour, more selective tracers can eliminate the problem.
Laboratory investigations
Laboratory investigations, although abnormal, are non-specific. The lack of characteristic laboratory abnormalities makes preoperative testing distinctly in accurate in most cases. Elevated serum bilirubin and alkaline phosphatase suggest biliary tract obstruction. Tumour marker such as CEA and CA 19—9 are occasionally elevated raising the suspicion of malignancy.
TREATMENT
Treatment in individual patients depends upon the mode of presentation, patient and tumour factors. Patient factors influencing the choice of treatment are age, nutritional status, performance status and the cardiopulmonary, hepatic and renal functions of the patient. Tumour factors determining the therapy are related to the stage and extent of disease (i. e. hepatic, colonic, duodenal and vascular invasion). Options of treatment are outlined below.
Surgery
The only potentially curative therapy remains surgical resection. Unfortunately, most patients found to have CaGB have unresectable disease-only 10-30% of patients being resectable on presentation. To simplify management guidelines patients can be divided into three clinical groups:
- Incidentally discovered CaGB during laparotomy or after cholecystectomy for benign disease.
- CaGB suspected or confirmed preoperatively on clinical or diagnostic workup.
- Advanced CaGB apparent on clinical or preoperative investigation findings.
Surgical options include:
(a) Simple cholecystectomy.
(b) Cholecystectomy with pericholedochal lymphadenectomy or extensive lymph node dissection at the coeliac axis and aorta (Radical cholecystectomy).
(c) Cholecystectomy with wedge resection of the liver bed (segments IV and V).
(d) Cholecystectomy with resection of hilum and common bile duct with biliary reconstruction.
(e) Cholecystectomy with pancreaticoduodenectomy.
(f) Cholecystectomy with right hepatic lobectomy with or without extension to segment IV.
(g) Total hepatectomy with orthoptic liver transplantation.
Incidentally discovered CaGB during laparotomy or after cholecystectomy for benign disease
Carcinoma of the gall bladder is incidentally discovered during cholecystectomy for benign disease in 12-36% of patients. If CaGB is discovered during surgery, the surgeon should decide whether curative surgery is possible after determining the extent of disease. If the disease is so extensive as to preclude curative resection then a biopsy along with the appropriate palliative procedure may be carried out.
The diagnosis of subclinical or occult CaGB is usually made after the excised specimen is opened after removal or by the pathologist during examination of the specimen. The gall bladder should, ideally, be Opened after its removal and examined carefully for any suspicious lesion before closing the abdomen. Doubtful specimens should be sent for immediate frozen section examination to determine the diagnosis and assess the depth of tumour invasion. If the tumour has not invaded beyond the muscle layer (pTl), simple cholecystectomy appears to be adequate. The 5-year survival of these patients is close to 100%.
If the tumour invades beyond the muscle layer of infiltrates perimuscular connective tissue (pT2), further surgery in the form of extended cholecystectomy is required. Simple cholccystectomy may be sufficient only when the tumour is located on the peritoneal aspect of the gallbladder without any contact with adjacent organs. For lesions adjacent to liver, extended cholecystectomy is required because of the increased chance of liver involvement.32,42 This, so called, extended or radical cholecystectorny involves en bloc removal of the gallbladder and a 2 cm or greater wedge resection of the gallbladder bed. The lymphatics surrounding the portal vein, hepatic artery, porta hepatis and the nodes behind the second part of the duodenum, of pancreas and coeliac axis are also dissected. The extent of liver resection ranges from a nonanatomical wedge resection to removal of segments IV & V, Segments IV, V and VIII and even right hepatic lobectomy.
Gallbladder cancer suspected or confirmed preoperatively on clinical and diagnostic workup.
The surgical management of CaGB diagnosed preoperatively and in patients fit to withstand surgery depends on the investigations and the subsequent laparotomy findings. Patients with organ-confined disease are treated by extended or radical cholecystectomy.42 There are reports of 5- year survival of 29% after extended cholecystectomy in patients with transmural (T3, T4) tumour invasion and lymph node involvement as compared to no survivors after simple cholecystectomy in this group of patients.
Criteria of resectability can vary but, if the following are present, surgical resection is contraindicated
- Multiple liver metastases.
- Ascites.
- Multiple peritoneal metastases.
- Distant metastases.
- Extensive involvement of hepatoduodenal ligament.
- Encasement or occlusion of major vessels.
- Poor performance status.
Direct involvement of colon, duodenum or liver is not absolute contraindications to surgery.
Advanced CaGB apparent on clinical and investigation finding
In patients not fit for tumour resection, some form of palliative procedure may be employed, such as bilio-enteric bypass or endoscopic/ percutaneous stenting in patients with obstructive jaundice.
Since the level of tumour Obstruction is usually at the common hepatic duct or above, the round Ligament approach to the segment III duct along with biliary enteric anastomosis provides good palliation. In the presence of tumour invasion of the umbilical fissure of the liver, segment III duct bypass is not possible and recourse has to be taken for an alternative approach such as the Longmire procedure.
Dramatic advances in the last decade, in both endoscopic and radiologically guided percutaneous stenting, have made operative bypass, in cases of unresectable cancers, largely unnecessary. For patients with distal common bile duct obstruction, an endoscopically placed stents provides both internal, and, if necessary, external drainage. It is rare for such patients to live long enough to require stent replacement because of sludge deposition. Duodenal or intestinal bypass may be performed as a palliative procedure if gastrointestinal obstruction is present.
Many Japanese surgeons have reported that aggressive surgery improves the outcome of patients with gallbladder cancer. Differences in survival rates between Japan and other countries have been noted.45 However, the extent of hepatic and lymph node resection, the need for resection of the extra hepatic ducts in nonjaundiced patients, the role of vascular resection, and the advisability of hepatopancreatoduodenectomy remain a matter of debate. Although no data from prospective, randomized studies are available, resection of the gallbladder and adjacent liver with or without the extra hepatic bile ducts and with a regional lymph node dissection is the operative approach recommended for selected patients with gallbladder cancer.
Cholecystectomy will prevent CaGB but all persons with asymptomatic gallstones need not, cannot and should not be advised to have prophylactic cholecystectomy to prevent CaGB. Those who have a higher risk of developing CaGB need to be identified and probably offered ‘preemptive’ cholecystectomy47. This will take age, geography, race, size of stone and stone / gallbladder volume ratio into account. Tumor markers and genetic markers may also help to identify these persons.
Radiotherapy
Radiotherapy has been used primarily as an adjuvant treatment following surgery. The 3 year cumulative survival rate was 10.1% for patients receiving intraoperative radiotherapy after resectional surgery whereas it was nil for a similar group of patients undergoing resection alone.49 External radiotherapy has shown some survival benefit.50 However, carcinoma gallbladder is not only relatively radio resistant but also the proximity of sensitive normal tissues limits the delivery of large doses of radiotherapy.
Chemotherapy
5 Fluorouracil (5-FU) either alone or in combination has been widely used but offers no survival benefit. However, hepatic arterial infusion of mitomycin C with or without systemic 5FU was associated with increased survival rates.51 Further studies are required before the routine use of adjuvant chemotherapy for CaGB can be recommended. Palliative chemotherapy for Nevin stage IV and V is not recommended as standard care.
DISCUSSION
Carcinoma of the gall bladder was regarded as uncommon at one time. But reports within the last 50 years have shown that it is not as rare as was previously supposed. Probably many tumours were not recognized and diagnosed during the course of treatment. Carcinoma of the gall bladder is the most common malignant tumour of the biliary tract. It accounts for 5% of all cancers found at autopsy. It ranks fifth in frequency of all gastrointestinal malignancy. Overall outcome of this disease is poor. Patients with gallbladder carcinoma have an overall mean survival rate of 6 months, and the 5 years survival rate is 5%53. However, its clinicopathological pattern, feasibility and prospects of different modalities of treatment were not evaluated on our country. In the present study, I have presented 50 cases of carcinoma of gall bladder from BSMMU, Dhaka over a period from September, 2008 to August, 2009.
It is the purpose of this small study to present 50 cases of carcinoma of gall bladder to show age and sex related incidence of malignancy with comprehensive picture of clinical aspect of the disease. It must be mentioned that this was very small study and may have limited epidemiological significance in certain aspects. In addition to the main objective, this series gives us the opportunity to study the following aspects of gall bladder disease:
In this series, patients of different age groups are included, ranging from 35 to 80 years of age. The highest incidence is recorded in their 5th and 6th decades in this study. Nagata et al and de-Aretxabala et al reported highest incidence in their 6th decade Jones and Maibenco et al showed that gallbladder carcinoma is diagnosed most frequently in individuals between ages 70 and 75 years• This study differs to some extent from the other studies.
The present study showed that the youngest patient suffering form carcinoma of the gallbladder is 35 years old lady. Tanga and Ewing showed that the youngest patient was of 43 years58. Maria et al showed 41 years. The youngest patient reported by Petcher, who found an 11 year old Navajo girl with carcinoma of gallbladder.
Overall, carcinoma of gall bladder was found more common in females (72%) than in males (28%) with female to male ratio is 2.57:1. The result is, more or less, consistent with the findings of other studies, in which it is 3:1. In a study, the ratio was 1.5:1.
We observed the clinical features of all the cases. Pain in the right hypochondrium was the most common presenting symptom in this study (Table 3.2) which correlates with the finding of Huber et al.60. In this study, 78% patients having carcinoma of gallbladder presented with persistent right upper abdominal pain, which resembles cholelithiasis. In one study, Cunningham et al have shown that 48.2% of patients of carcinoma of gallbladder had a preoperative diagnosis of symptomatic cholelithiasis.
Anaemia was present in 39 patients (78%). Gallbladder was palpable in 25 patients (50%), while jaundice was present in 20 patients (40%). Weight loss was found in 34 patients (68%), which ranks as one of the two commonest symptoms. Different studies showed that anorexia, weakness, vomiting, weight loss, palpable upper right abdominal mass, jaundice and hepatomegaly were found in different combinations and in varying percentage among the cases diagnosed as carcinoma of gallbladder. The clinical features noted in the present series were also nonspecific as carcinoma of gallbladder does not present any definite clinical signs and symptoms.
Jaundice is an important clinical feature. It was present in 40% patients. The study of Nagata et a1 showed a lower incidence (35%). Among laboratory investigations, Serum alanine aminotransferase was found elevated in 38 patients (76%). Serum Alkaline Phosphatase was raised in 23 patients (46%). Prothrombin time was prolonged in 19 patients (38%). Increased level of the enzymes corresponds with the severity of jaundice and biliary obstruction.
Ultrasonogram (USG) of the hepatobiliary system and the pancreas was done in all patients. This study shows that USG was positive for gallstones in 76% of patients. Soft tissue mass was detected in 35 patients (70%); most of them was in fundal region of the gall bladder.
In a study, solid mass in the gallbladder region was detected on USG in 50.84% of gallbladder carcinoma, thickened gallbladder wall in 44.06% and intraluminal polypoid mass in 5.08% cases, with an overall positive result in almost 100% cases. Also Cubertaford et al reported the value of USG in diagnosing carcinoma of the gallbladder with sensitivity of about 64%. Another study reveals the diagnostic accuracy of USG is over 80% in detecting carcinoma of gallbladder. All these results are, more or less, close to the reported data in this study.
CT scan was done in 20 patients. Gallbladder mass could be detected in all cases (100%). Moreover, liver metastases and gall stone were detected in 14 patients(70%),lymphnode was found in 5 cases(15%).Though Araki et al showed 60% sensitivity of gallbladder carcinoma in CT scan. This difference may be because we were selective in investigating the patients with CT scan and only USG-confirmed cancer patients were sent for the scan.
In this study most of the patients presented with advanced disease. Fifteen patient (30%) under went complete resection. Among them only cholecystectomy could be done only in 12 patients (24%), Radical chotecystectomy was done only in 3 patients (6%). Though Hiromichi et al showed 38% under went complete resection among them 20.8% was simple cholecystectomy and 17.2% was radical cholecystectomy. This difference may be because most of our patient present late.
In this study, 87.5% patients of carcinoma gallbladder proved to have adenocarcinoma, the rest (12.5%) of the patients has squamous cell carcinoma showing similarity with the different studies. Similar study done by Maria et al on 61 patients and was diagnostic in all the cases having adenocarcinoma. Strauch et al showed 82% adenocarcinoma, 7% undifferentiated, 3% squamous cell carcinoma and remaining other rare vaneties.
In the present study, it is showed that gallbladder cancer is a disease of aged female patient as is the case in gall stone disease. Clinical features do not follow any definite features. USG is able to detect soft tissue mass in the gallbladder, metastases to liver or ascites of that advanced disease. So, the only confirmatory diagnosis is possible by laparotomy and biopsy. As there is negligible role of chemotherapy and radiotherapy, the prognosis is poor, if the disease is not diagnosed early. Most of the patient in the study presented late and with advanced disease. So, we could offer very little to their ultimate cure in this hospital.