Hypertension is the largest and commonest risk factor for cardiovascular diseases, growing in prevalence and poorly controlled virtually everywhere and is still largely ignored as a public health problem in most developing countries 1,2 .
High blood pressure also known as hypertension is called the “silent killer” because it doesn’t have symptoms and thus many people are not aware that they have this condition3.
Globally, 7 million people die and 1.5 billion suffer every year because of high blood pressure or hypertension4. As per statistics, there was an estimated 972 million people suffering from hypertension in the year 2000 and by 2025, it is estimated that around 1.56 billion people will have it. High blood pressure is a major risk factor for stroke, coronary heart disease, heart and kidney failure. The higher the pressure, the greater the risk and lower the expectation of life. Intensive research carried out during the past few years, aiming at the control of hypertension at the community level, has already provided valuable results. The studies have shown that control of hypertension in a population is feasible and that it can be carried out through the existing system of health services in different countries. This control of blood pressure leads to a reduction of complications caused by high blood pressure. The World Health Organization attributes hypertension, or high blood pressure, as the leading cause of cardiovascular mortality. The World Hypertension League (WHL), an umbrella organization of 85 national hypertension societies and leagues, recognized that more than 50% of the hypertensive population
worldwide is unaware of their condition. To address this problem, the WHL initiated a global awareness campaign on hypertension in 2005 and dedicated May 17 of each year as World Hypertension Day (WHD). Over the past three years, more national societies have been engaging in WHD and have been innovative in their activities to get the message to the public. In 2007, there was record participation from 47 member countries of the WHL. During the week of WHD, all these countries — in partnership with their local governments, professional societies, nongovernmental organizations and private industries — promoted hypertension awareness among the public through several media and public rallies. Using mass media such as Internet and television, the message reached more than 250 million people. As the momentum picks up year after year, the WHL is confident that almost all the estimated 1.5 billion people affected by elevated blood pressure can be reached. The success of WHD is due to the enthusiasm and voluntary action of multiple stakeholders from every member country5. In 2005, as the inaugural effort, the theme was simply ‘Awareness of high blood pressure’. The 2006 theme was ‘Treat to goal’, with a focus on keeping blood pressure under control. The recommended blood pressures are less than 140/90 mmHg for the general population and for the hypertensive population without any other complications, and less than 130/80 mmHg for those with diabetes mellitus or chronic kidney disease. These are the cut-off values recommended by international and Canadian guidelines6. The 2007 WHD theme was ‘Healthy diet, healthy blood pressure’. Through such specific themes, the WHL intends to raise awareness not only of hypertension, but also of factors contributing to an increase in the incidence of hypertension and on ways to prevent it. In an effort to empower the public, the theme for 2008 was ‘Measure your blood pressure…at home’. Recent reports confirm the ease, accuracy and safety of blood pressure measurements using home
monitors. The Theme for 2010 was Healthy Weight – Healthy Blood Pressure.. The theme for 2011 is Know Your Numbers and Target Your Blood Pressure.
Persons with hypertension are at increased risk for a number of serious complications, including coronary heart disease, stroke, congestive heart failure and renal dysfunction and is one of the major risk factors for cardiovascular mortality, which accounts for 20-50% of all deaths7,8.
Prevention is possible, although rarely achieved, and treatment can lead to a reduced incidence of complications, including stroke, coronary heart disease, heart failure, and kidney disease. By 2030, 23 million cardiovascular deaths are projected, with 85% occurring in low- and middle-income countries9.
In 2000, according to the World Health Report 2002, the number of people worldwide afflicted with hypertension was about 600 million. Hypertension is estimated to cause 7.1 million deaths annually, about 13% of the total global deaths. Since most blood pressure-related deaths or nonfatal events occur in middle age or among the elderly, the loss of life years comprises a smaller proportion of the global total, but is nonetheless substantial (64.3 million DALYs, or 4.4% of the total). As countries at different levels of development have been progressing through different stages of health transition at different rates, the socioeconomic gradients with hypertension vary. Blood pressure levels and hypertension have been proven to be inversely related to socioeconomic status in developed countries, but in the developing world such correlations have not always been evident.
Health promotion based on societal knowledge and perceptions regarding chronic diseases such as diabetes and hypertension are considered to be an essential component of any strategy that aims at disease control and prevention10. Awareness alone is obviously not enough to improve cardiovascular health, but it is a prerequisite for making the right decisions with regard to health. Studies showed that knowledge regarding risk factors of hypertension among the urban and rural areas varies. To promote effective health management and to implement future protection programs, it is important for health professionals to recognize the level of awareness among the population with regard to hypertension, and the sources of relevant medical information. In this study the main objective was to compare the level of knowledge about risk factors of hypertension between urban and rural community. This study was conducted in Natunbazar of Kallyanpur area of Dhaka city and Biramerkandi village of Kotalipara upazila of Gopalgonj district.
Background
In developed countries, the major burden of disease is due to chronic diseases, such as heart disease and stroke. In contrast, the major burden of disease among people in developing countries has been due largely to diseases caused by malnutrition, poor sanitation and infection. In recent years, with increasing economic and demographic development, there has been a shift in developing countries from diseases caused by poverty towards chronic, non-communicable, lifestyle-related diseases. The rapid emergence of these chronic diseases has not occurred with a similarly rapid decline in infectious diseases. Therefore, these developing countries are experiencing high rates of both infectious and chronic diseases. 2. The increase in chronic diseases in developing countries has been brought about by the increasing prevalence of risk factors, such as increased alcohol consumption, smoking, obesity, physical inactivity and low fruit and vegetable intake. In parallel with this, there is also increased evidence of high blood pressure and high cholesterol levels. 3. The preventive strategies required to reverse this trend for these emerging diseases include the education of public health professionals, the introduction of surveillance activities to monitor changes in risk factors, the introduction of health promotion, the development of prevention research and improved advocacy for disease prevention programmes. Experience from other countries provides evidence that prevention programmes can work. The global challenge is to ensure that implementation of such programmes in the world’s developing nations does not come too late11.
Hypertension is the term used to describe high blood pressure. Blood pressure is a measurement of the force against the walls of your arteries as the heart pumps blood through the body. Blood pressure readings are measured in millimeters of mercury (mmHg) and usually given as two numbers – for example, 120 over 80 (written as 120/80 mmHg). One or both of these numbers can be too high12.
Overview of Hypertension13
Hypertension is one of the most common worldwide diseases afflicting humans. Because of the associated morbidity and mortality and the cost to society, hypertension is an important public health challenge. Over the past several decades, extensive research, widespread patient education, and a concerted effort on the part of health care professionals have led to decreased mortality and morbidity rates from the multiple organ damage arising from years of untreated hypertension.
The heart pumps blood into the arteries with enough force to push blood to the far reaches of each organ from the top of the head to the bottom of the feet. Blood pressure can be defined as the pressure of blood on the walls of the arteries as it circulates through the body. Blood pressure is highest as its leaves the heart through the aorta and gradually decreases as it enters smaller and smaller blood vessels (arteries, arterioles, and capillaries). Blood returns in the veins leading to the heart, aided by gravity and muscle contraction.
Pathophysiology
The pathogenesis of essential hypertension is multifactorial and highly complex. Multiple factors modulate the blood pressure (BP) for adequate tissue perfusion and include humoral mediators, vascular reactivity, circulating blood volume, vascular caliber, blood viscosity, cardiac output, blood vessel elasticity, and neural stimulation. A possible pathogenesis of essential hypertension has been proposed in which multiple factors, including genetic predisposition, excess dietary salt intake, and adrenergic tone, may interact to produce hypertension. Although genetics appears to contribute to essential hypertension, the exact mechanism has not been established.
The natural history of essential hypertension evolves from occasional to established hypertension. After a long invariable asymptomatic period, persistent hypertension develops into complicated hypertension, in which target organ damage to the aorta and small arteries, heart, kidneys, retina, and central nervous system is evident. The progression begins with prehypertension in persons aged 10-30 years (by increased cardiac output) to early hypertension in persons aged 20-40 years (in which increased peripheral resistance is prominent) to established hypertension in persons aged 30-50 years, and, finally, to complicated hypertension in persons aged 40-60 years.
One mechanism of hypertension has been described as high-output hypertension. High-output hypertension results from decreased peripheral vascular resistance and concomitant cardiac stimulation by adrenergic hyperactivity and altered calcium homeostasis. A second mechanism manifests with normal or reduced cardiac output and elevated systemic vascular resistance due to increased vasoreactivity. Another (and overlapping) mechanism is increased salt and water reabsorption (salt sensitivity) by the kidney, which increases circulating blood volume.
Hypertension is a lifelong disorder. For optimal control, a long-term commitment to lifestyle modifications and pharmacological therapy is required. Therefore, repeated in-depth patient education and counseling not only improve compliance with medical therapy but also reduce cardiovascular risk factors.
Definition of blood pressure:
Blood pressure is the force applied against the walls of the arteries as the heart pumps blood through the body.
Blood pressure number:
The first number, systolic blood pressure measures the maximum pressure exerted as the heart contracts. A measurement over 90 and under 140 is generally considered normal for an adult. The lower number indicates diastolic pressure is a measurement taken between beats, when the heart is at rest. A measurement over 60 and under 90 is generally considered normal for an adult.
In 90% of people with hypertension, the cause of high blood pressure is not known and is referred to as primary or essential hypertension. While the specific cause is unknown.
Factors that can not be changed
Age: The older a person is, the greater the likelihood that he or she will develop high blood pressure, especially elevated systolic readings. This is largely due to arteriosclerosis, or “hardening of the arteries.”
Race: African Americans develop high blood pressure more often than Caucasians. They develop high blood pressure at a younger age and develop more severe complications sooner in life.
Socioeconomic status: High blood pressure is found more commonly among the less educated and lower socioeconomic groups. Residents of the southeastern United States, both Caucasian and African American, are more likely to have high blood pressure than residents of other regions.
Family history (heredity): The tendency to have high blood pressure appears to run in families.
Gender: Generally men have a greater likelihood of developing high blood pressure than women. This likelihood varies according to age and among various ethnic groups.
Factors that can be changed
Obesity: As body weight increases, the blood pressure rises. Obesity is defined as having a body mass index (BMI) greater than 30 kg/m. A BMI of 25-30 kg/m is considered overweight (BMI=weight in pounds x 703/ height in inches) Being overweight increases the risk of high blood pressure. Health care practitioners recommend that all obese people with high blood pressure lose weight until they are within 15% of their healthy body weight.
Obese people are two to six times more likely to develop high blood pressure than people whose weight is within a healthy range.
Not only the degree of obesity is important, but also the manner in which the body accumulates extra fat. Some people gain weight around their belly (central obesity or “apple-shaped” people), while others store fat around their hips and thighs (“pear-shaped” people). “Apple-shaped” people tend to have greater health risks for high blood pressure than “pear-shaped” people.
Sodium (salt) sensitivity: Some people have high sensitivity to sodium (salt), and their blood pressure increases if they use salt. Reducing sodium intake tends to lower their blood pressure. Americans consume 10-15 times more sodium than they need. Fast foods and processed foods contain particularly high amounts of sodium. Many over-the-counter medicines also contain large amounts of sodium. Read food labels and learn about salt content in foods and other products as a healthy first step to reducing salt intake. Fast food restaurants also make the salt and calorie content of their food available to consumers at their restaurants,
Alcohol use: Drinking more than one to two drinks of alcohol per day tends to raise blood pressure in those who are sensitive to alcohol.
Birth control pills (oral contraceptive use): Some women who take birth control pills develop high blood pressure.
Lack of exercise (physical inactivity): A sedentary lifestyle contributes to the development of obesity and high blood pressure.
Medications: Certain drugs, such as amphetamines (stimulants), diet pills, and some medications used for cold and allergy symptoms such as pseudoephedrine, tend to raise blood pressure.
Symptoms of Hypertension
Most of the time, there are no symptoms. Symptoms that may occur include:
- Confusion
- Ear noise or buzzing
- Fatigue
- Headache
- Irregular heartbeat
- Nosebleed
- Vision changes
Prevention of Hypertension
Adults over 18 should have their blood pressure checked routinely. Lifestyle changes may help control your blood pressure:
- Avoid smoking. (See: Nicotine withdrawal)
- Do not consume more than 1 drink a day for women, 2 a day for men.
- Eat a diet rich in fruits, vegetables, and low-fat dairy products while reducing total and saturated fat intake (the DASH diet is one way of achieving this kind of dietary plan). (See: Heart disease and diet)
- Exercise regularly. If possible, exercise for 30 minutes on most days.
- If you have diabetes, keep your blood sugar under control.
- Lose weight if you are overweight. Excess weight adds to strain on the heart. In some cases, weight loss may be the only treatment needed.
- Try to manage your stress.
One can lower systolic blood pressure (the top number) by 8 to 14 points by switching to the DASH diet. The DASH diet is based on 2,000 calories a day. It’s high in fruits, vegetables, legumes, whole grains, and low-fat dairy. It’s low in fat. For those over age 50, a systolic blood pressure higher than 140 is a greater risk factor for heart disease than the diastolic blood pressure (lower number).
Symptoms for consultain hypertension:
- Chest pain
- Confusion
- Excessive tiredness
- Headache
- Nausea and vomiting
- Shortness of breath
- Significant sweating
- Vision changes
RATIONALE
The World Health Organization attributes hypertension, or high blood pressure, as the leading cause of cardiovascular mortality, growing in prevalence and poorly controlled virtually everywhere and is still largely ignored as a public health problem in most developing countries. The World Hypertension League (WHL), recognized that more than 50% of the hypertensive populations worldwide are unaware of their condition.
Persons with hypertension are at increased risk for a number of serious complications, including coronary heart disease, stroke, congestive heart failure and renal dysfunction and are one of the major risk factors for cardiovascular mortality, which accounts for 20-50% of all deaths.
Health promotion based on societal knowledge and perceptions regarding chronic diseases such as diabetes and hypertension are considered to be an essential component of any strategy that aims at disease control and prevention.
To promote effective health management and to implement future protection programs, it is important for health professionals to recognize the level of awareness among the population with regard to hypertension, and the sources of relevant medical information.
This study will be able to identity the level of knowledge about risk factors and complication of hypertension between urban & rural population. It will determine differences the level of knowledge among the population. The study findings will help to take appropriate preventive and control measure for hypertension for urban & rural population. Which will ultimately undue the mortality and morbidity from this chronic disease.
Research question:
What is the level of knowledge of risk factors of hypertension and its complication between rural and urban population?
Objectives of the study:
General Objective:
To assess and compare the level of knowledge regarding risk factors of hypertension and its complication among the urban and rural population
Specific objectives:
- To assess the level of knowledge about hypertension
- To assess the level of knowledge about the risk factors of hypertension
- To assess the level of knowledge about complications of hypertension
- To Compare the level of knowledge of hypertension and its complication between rural and urban population
- To determine the socio-economic characteristic of the respondents
CONCEPTUAL FRAMEWORK
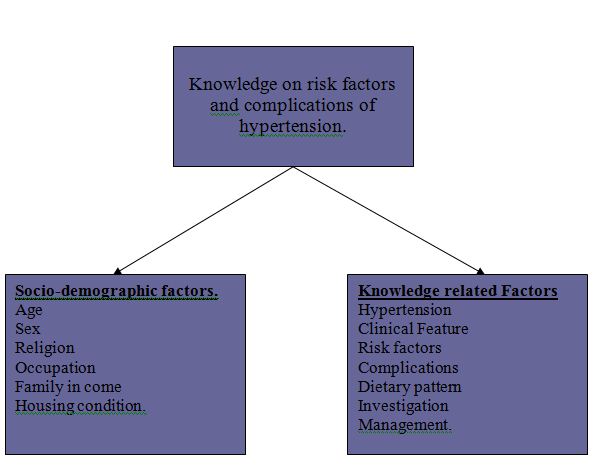 VARIABLES
VARIABLES
Socio-demoeraphic variables
- Age
- Sex
- Religion,
- Occupation
- Family income.
Knowledge related variables
- Hypertension,
- Clinical Feature
- Risk factors, Complications
- Dietary pattern
- Investigation,
- Management
OPERATIONAL DEFINITIONS
Age: Age of the respondents of more than 30 years as stated by the respondents.
Occupation: The job/Work the way in which she/he is presently spending time irrespective of gainful or gain less.
Type of activity: Person does physical activity in terms of Mild, Moderate and Vigorous on the basis of minimum activity hour.
Risk factor: Risk factor is a variable associated with an increased risk of disease or infection.
Complication: An unfavorable evolution of a disease, a health condition or a medical treatment.
Management is a collaborative process that facilitates recommended treatment plans to assure the appropriate medical care is provided to disabled, ill or injured individuals.
Prevention: To avoid doing; stay away from dangerous or risky things.
LITERATURE REVIEW
Literatures related to knowledge on Risk Factors and Complications of Hypertension were searched and collected. Review of available printed documents, reports; thesis, books, journals, internet searches for the electronic resources were done. Internet search through Google and the home pages of WHO and others were carried out.
Unsatisfactory blood pressure (BP) control so often described in treated hypertensive populations is also explained by insufficient physicians’ awareness of experts’ guidelines. We assessed awareness of current recommendations about hypertension management in a general practice setting, using the World Health Organization/International Society of Hypertension (WHO/ISH) 1999 guidelines as reference. In a regionwide survey, a total of 5133 physicians (three-quarters of all active general practitioners in Lombardy, a region of north-western Italy) were contacted by letter and received a multiple choice 10-item questionnaire. Data on physicians’ demographic characteristics, information on hypertension prevalence and their perception of BP control among their patients were also requested in an additional form. The number of answers in agreement with WHO/ISH guidelines was used as an awareness measure. This was considered adequate if correct answers to six out of 10 questions, including an appropriate definition of hypertension, were provided. Of the 1256 returned questionnaires (a 24.5% response rate), 1162 were suitable for analysis. The mean score of correct answers was 5.3 points and only 20.1% of the study population correctly answered at least six of the questions (including that on the definition of hypertension in the elderly). Guidelines awareness was negatively related to increase in physicians’ age and duration of clinical practice and by the male gender. Finally, the physicians reported a high rate of achieved BP control, and those who were considered to have achieved highest rates (>75%) of control in their patients had a lower rate of adequate knowledge than those who reported less-successful therapeutic results (18 vs 25%, P<0.01), suggesting that they ignored or disregarded the goal BP recommended by the guidelines. This large regional survey shows that a sufficient degree of guidelines awareness is present in a minority of primary-care physicians in the Italian region of Lombardy. Therefore, further efforts are required to intensify information strategies for improving professional education, training and practice organization aimed at achieving therapeutic goals. Physicians with longer duration of clinical practice represent a particularly relevant target group for these interventions14.
One study evaluated the prevalence, awareness, and treatment of hypertension in Olmsted County, Minnesota, a community in which the incidence of stroke had been studied between the 1950s and the 1990s.Researchers examined 636 residents aged 45 years or older. Participants were considered to have high blood pressure if their systolic pressure was >140 mm Hg and their diastolic was >90 mm Hg. Of the people studied, 53%were diagnosed as having hypertension and of those only 39%knew of their condition. Of those with hypertension, 17%had been treated and the condition was considered to be under control; 28%had been treated but the hypertension was not yet under control.A spokesperson for the American Heart Association said that the study’s findings support the results of its own recent nationwide surveys. Compared with a similar study performed in 1993, fewer participants in the current study were aware that they had high blood pressure and, even with treatment, fewer had had their blood pressure controlled. In the 1993 study, by the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure, 68%were aware that they had high blood pressure, 53%were being treated for the condition, and in 27%the hypertension was controlled through treatment. A comparison with the figures from the recent study shows that there has been a substantial decline in the awareness of the condition15.
To determine the level of awareness of hypertension and pharmacological management in patients from a rural community of Australia a study was conducted by White, Wang and Jelinek16. A total of 665 patients were studied. The patients were recruited from Albury-Wodonga and surrounding districts, which are located in a rural area of south-eastern Australia. Demographic information and medical history were recorded for all patients. Clinical data were also recorded. Of the 665 patients, 449 (75%) were hypertensive, and of these 449 hypertensive patients, 195 (43.4%) were aware that they had hypertension. Blood pressure was inadequately controlled in 399 of the hypertensive patients (88.9%) according to the management guidelines of the National Heart Foundation of Australia. Of all the patients who had hypertension, 247 (55.0%) were not receiving antihypertensive therapy. Of those receiving therapy, 132 (65.3%) were being administered only one antihypertensive (monotherapy). The most commonly prescribed antihypertensive classes were angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, diuretics, –Mockers and calcium channel blockers.
To determine the prevalence and possible risk factors for hypertension and prehy-pertensive state in Trivandrum City of Kerala17 (South India) using Joint National Committee (JNC) VII criteria, a team of trained fourth year medical students conducted a 10% random household survey in certain wards of the City. Households were selected using a random start and interval and all the members above the age of 10 years were interviewed using a standard questionnaire. The blood pressure (BP) was measured twice in each participant and the mean value of the two measurements was taken. A total of 482 individuals (212 males and 270 females) were interviewed in the survey. Overall
prevalence of hypertension was 47% (n = 226) with equal sex ratio; 109 (21.6%) had stage-I hypertension, 45 (9.34%) had stage-II hypertension and 72 were taking drug treatment Only 55 (11.4%) individuals had normal BP, while 201 (41.7%) were prehypertensives. Only 81 (16.8%) hypertensive patients were aware of their disease. Among the parameters such as dietary habits, physical activity, educational standards, salt intake, and diabetes mellitus, only high salt diet (P= 0.03) and diabetes mellitus (P= 0.004) had a significant association with hypertensive state. In conclusion, the prevalence of hypertension is high but the awareness is low in our community, and intervention is necessary to impose control measures and to improve awareness.
In a study in USA18 , 33% of the hypertensive individuals were unaware of their condition. The awareness was low among the young, but increased with older age. The popular belief that hypertension and diabetes mellitus are diseases of the elderly may be the reason for the low level of awareness among the youth. Improving awareness in the community is an important population-based strategy for prevention of complications of these diseases.
None among the prehypertensive group was aware of predisposition to hypertension and requirement of life style and dietary modifications and blood pressure check-up at least annually. Vegetarian diet showed a trend towards a protective effect on hypertension in our study in contrast to an earlier observation in which mixed diet showed a protective effect19. The awareness of hypertension was higher among persons with higher educational status, in contrast to the observation from a recent study from Spain.
One study was conducted in Greece20 to see the prevalence of hypertension. The prevalence of hypertension (based on two arterial blood pressure measurements on a single occasion) was 40.2% for men and 38.9% for women (age-adjusted to the adult Greek population of 2001). In the sample examined, awareness among hypertensives is 54.4%, pharmaceutical treatment among those aware is 83.9%, and effective control among hypertensives is 15.2%. Prevalence of hypertension increases with age and is higher in rural areas and among individuals of lower education. Awareness and control of hypertension is higher among older individuals, among women and among the highly educated. Moreover, awareness of hypertension is higher among rural residents, whereas control of hypertension is more effective among urban residents.
One cross-sectional survey of 314 middle-aged subjects (163 men; age range 40-60 years, mean 49 years) was conducted in urban ThiruvananthapuramCity. Kerala, to estimate the prevalence of hypertension, examine its correlates, and assess the degree of awareness, treatment, and control of high blood pressure. Blood pressure was measured by a nurse graduate using a mercury column sphygmomanometer and a standardized technique. We used multivariable analyses to examine the sociodemographic and clinical correlates of hypertension. The overall prevalence of hypertension in our sample was 54.5% (men 56.3%, women 52.3%). The factors associated with an increased prevalence of hypertension were higher body-mass index (odds ratio for a value in the top tertile of 2.33, 95% confidence interval: 1.2-4.4), and older age (odds ratio for the age group 55-60 years of 2.65, 95% confidence interval: 1.3-5.6). An occupation involving moderate or greater physical activity was inversely associated with the prevalence of hypertension (odds ratio 0.35, 95% confidence interval 0.13-0.94). Among hypertensives, 39% were aware of the condition, while 29% were treated with blood pressure-lowering medications. Adequate control of elevated blood pressure was achieved in only 30.6% of treated hypertensives. In our community-based sample, over half of all middle-aged
individuals were hypertensive, but less than a third were under treatment. Adequate control of hypertension was achieved in less than a third of the treated individuals21.
To determine prevalence, awareness, treatment, and control of hypertension, and its risk factors in an urban Korean population a cross-sectional survey was conducted in Ansan-city, Korea. This Population-based samples of people aged 18-92 years in Ansan-city, Korea, were selected, yielding 2278 men and 1948 women, and their blood pressures were measured using a highly standardized protocol. Hypertension was defined as a systolic BP > or = 140 mniHg or diastolic BP > or = 90 mniHg or reported treatment with antihypertensive medications, and subclassified according to 1999 WHO-ISH guidelines. Isolated systolic hypertension (ISH) defined as a systolic BP > or = 140 mmHg and diastolic BP < 90 mmHg was also examined. Data were stratified by age and sex. The overall prevalence of hypertension in this study was 33.7%. Among these, 64.9% had Grade 1 hypertension, 22.5% Grade 2, and 12.5% Grade 3. Age-specific prevalence of hypertension increased progressively with age, from 14.19% in 18 to 24 year-olds to 71.39% in those 75 years or older. Hypertension prevalence was significantly higher in men (41.5%) than in women (24.5%) (P < 0.001). Isolated systolic hypertension had significantly lower prevalence (4.33%) within the population, although in the elderly aged 55 years or more it rose by 11.13%. Overall, 24.6% of hypertensive individuals were aware that they had high blood pressure, as much as 78.6% were being treated with antihypertensive medications, and 24.3% were under control. Hypertension awareness as well as treatment and control rates varied by sex, with women higher in all three rates. Multivariate analysis revealed that age, body mass index and abdomen circumference were significantly associated with prevalence of hypertension both in men and women22 .
Hypertension was undetected in almost one-half of all hypertensive Canadians surveyed, and only 13% of those with hypertension were treated and controlled to recommended blood pressure targets. The reasons for poor control are likely multifactorial; however, a lack of public awareness and understanding of hypertension may contribute to the epidemic of uncontrolled hypertension in Canada. A national telephone survey was conducted comprising 1001 randomly selected men and women older than 40 years of age to determine the level of public awareness, understanding and misconception of hypertension in Canada. The survey was balanced for region, age and sex. Thirty-four per cent of respondents had been diagnosed with high blood pressure or hypertension by a health care professional, but only 58% of respondents had ever discussed their blood pressure with a physician, and only 44% were able to identify their own blood pressure or differentiate blood pressure levels considered to be above or below recommended targets. Overall, respondents had a poor understanding of the consequences of high blood pressure or hypertension. The majority were unaware of the association between hypertension and heart disease (80%), heart attack (66%), kidney disease (98%), damage to blood vessels (95%) and premature death (74%). Respondents also had limited knowledge of lifestyle issues affecting hypertension, despite 44% indicating that they were overweight and 18% identifying themselves as smokers. Almost two-thirds (63%) thought hypertension had clearly identifiable signs or symptoms, although they believed that hypertension was not a serious medical condition. Most respondents (59%) falsely believed that they would not develop hypertension and 38% thought that they would be able to control hypertension without the aid of a physician if they did have hypertension23.
To assess knowledge and perceptions about hypertension among migrants in Delhi, India a cross-sectional study was conducted by Kusuma, Gupta and Pandav24. Neo-migrants were selected from different slums and work sites. All participants were randomly chosen. Blood pressure measurements (three) were taken by trained staff. Participants responded to a questionnaire first developed in English and translated to Hindi. Questionnaire assessed knowledge about hypertension, treatment, and prevention. A total of 226 settled migrants and 227 neo-migrants were surveyed. Obesity and hypertension were more common among settled migrants. Hypertension prevalence was not significantly different by migration category (settled men had the highest prevalence, 25%). The term “blood pressure” is used by both groups to refer to hypertension (even in Hindi). Eighteen percent and 13% of neo-migrants and settled migrants stated that hypertension means dizziness, respectively. Perception that hypertension is a serious problem was significantly lower among neo-settled migrants (58% vs 70%). Most respondents in both groups cited tensions/anger as the main reason for hypertension. None of the neo-migrants and only 4% of the settled migrants cited tobacco as a cause of hypertension. Forty-six percent of neo-migrants and 48% of settled migrants recognized that hypertension can be prevented.
A Cross-sectional telephone survey was conducted by Sanne S25 and associates among 296 adults suffering from hypertension revealed that eighty-nine percent of respondents were Black, 79% were female, 75% had a monthly income ,$1000, and 62% had completed high school. Items with the lowest percentage of correct responses included knowing that hypertension does not cause cancer (41.9% correct), a blood pressure of 130/80 mm Hg is normal (59.8% correct), hypertension lasts a lifetime (60.5% correct), and renal failure is a complication of hypertension (76.4% correct). Overall, 39%
answered 9 or 10 questions correctly. Low hypertension knowledge (#7 questions correct) was associated with age 60 years, having less than a high school education, and reporting a first hypertension diagnosis within 9 years before being surveyed. The study concluded that hypertension knowledge deficits in specific content areas and among certain subgroups were present in this urban population. Educational programs focusing on newly diagnosed hypertensive patients and aimed at filling targeted knowledge deficits may be a cost-effective approach to increase hypertension knowledge in similar populations.
Study in Vietnum conducted by Kishimoto et al26 among 155 rural Vietnamese, 147 urban Vietnamese, and 102 urban Japanese subjects, and 159 Japanese outpatients. The respondents were asked to identify the risk factors for diabetes and hypertension and their sources of medical information by answering multiple-choice questions. This study revealed that excessive sweet intake, lack of exercise, and obesity were cited as risk factors for diabetes by the urban Vietnamese and Japanese subjects. The most commonly cited risk factor for hypertension by the Japanese subjects was excessive salt intake, whereas obesity and alcohol consumption were cited by the urban and rural Vietnamese subjects, respectively. In both countries, medical information was mainly obtained from medical staff, but other mass media were also commonly used as sources of information. Among the 155 rural Vietnamese subjects, 18 (11.6%) were hypertensive, and 7 (38.9%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. The rural Vietnamese subjects considered excessive alcohol consumption (87.1%), obesity (83.9%), and smoking (80.6%) as the 3 major risk factors for hypertension, and 70.3% of these people identified excessive salt intake, which ranked seventh among the 9 factors listed in the questionnaires, as a risk for hypertension (Figure 2a). Among the 147 urban Vietnamese subjects, 33 (22.4%) were hypertensive, and 11 (33.3%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. The urban Vietnamese subjects considered obesity (79.6%), aging (78.9%), and excessive alcohol consumption (77.6%) to be the 3 major risk factors for hypertension. Although 66.7% of the urban Vietnamese subjects identified excessive salt intake as a risk factor for hypertension, it was ranked eighth among the 9 factors listed in the questionnaires. Among the 102 urban Japanese subjects, 13 (12.7%) were hypertensive, and 10 (76.9%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. In all, 80.4% of the urban Japanese subjects considered excessive salt intake as a risk factor for hypertension, which was the most frequently selected choice among the listed risk factors. Among the 159 Japanese outpatients, 58 subjects (36.5%) were hypertensive, and 49 (84.5%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. In all, 69.8% of the Japanese outpatients considered excessive salt intake as a risk factor for hypertension; it was the most frequently selected option among the listed risk factors. The patterns of the results for all the patients and for the hypertensive patients were quite similar.
To describe trends in the prevalence, awareness, treatment, and control of hypertension in the United States a study was conducted by Hajjar and Kotchen27 using NHANES data in 1999-2000, 28.7% of NHANES participants had hypertension, an increase of 3.7% (95% confidence interval [CI], 0%-8.3%) from 1988-1991. Hypertension prevalence was highest in non-Hispanic blacks (33.5%), increased with age (65.4% among those aged >60 years), and tended to be higher in women (30.1%). In a multiple regression analysis, increasing age, increasing body mass index, and non-Hispanic black race/ethnicity were independently associated with increased rates of hypertension. Overall, in 1999-2000,
68.9% were aware of their hypertension (no significant decline of -0.3%; 95% CI, – 4.2% to 3.6%), 58.4% were treated (increase of 6.0%; 95% CI, 1.2%-10.8%), and hypertension was controlled in 31.0% (increase of 6.4%; 95% CI, 1.6%-11.2%). Women, Mexican Americans, and those aged 60 years or older had significantly lower rates of control compared with men, younger individuals, and non-Hispanic whites.
Methodology:
Study Design
This was a cross-sectional study.
Study Area & Population
This study was conducted in Natunbazar of Kallyanpur area of Dhaka city and Biramerkandi village of Kotalipara upazila of Dhaka district.
Study Period
The study period was from May 2011- January 2012
Sample Size
Selection Criteria
Inclusion Criteria
• Permanent residence of the study area
• All male and female of more than 30 years of age irrespective of religion and customs.
• Those who are willing to participate in the study
Exclusion criteria
• Physically and mentally handicapped
Research Instruments:
The following research instruments were used in data collection:
Questionnaire: The questionnaire included the information so as to elicit socio-demographic information (age, gender, occupation, religion, income, housing type), to assess and compare the level of knowledge regarding risk factors of hypertension (type of physical activity, vegetable consumption, extra dietary salt intake, Smoking habit) and its complication (coronary heart disease, stroke, congestive heart failure and renal dysfunction and cardiovascular mortality).
Data Collection Procedure:
Data was be collected through face to face interview.
Knowledge level scoring:
To assess the level of knowledge, one scoring system was adopted. There are nine knowledge related questions. Each question has some options. According to the number
of options mentioned by the respondents, against one question a score was given. Summing the total scores was made percentage against total number of options of all nine questions. Then the score was graded as follows;
Poor <40%
Moderate 40%-60%
Satisfactory 60%- 80%
Excellent 80%-100%
Data Processing and Analysis:
After the completion of data collection, data will be edited, coded and entered in computer. Frequency tables of socio-demographic characteristics and cross tables with test of significant among knowledge level and socio-demographic characteristics were also done using appropriate SPSS software.
Ethical consideration:
Before data collection objective of the study was informed to the respondent and requested to participate in the study.
Informed consent was taken from the participants of the study
The privacy and confidentiality were strictly maintained during data collection.
RESULT:
This current study was conducted to compare the level of knowledge among urban and rural population on risk factors and complications of hypertension. Study samples were total 402
Distribution of respondents by Educational Status
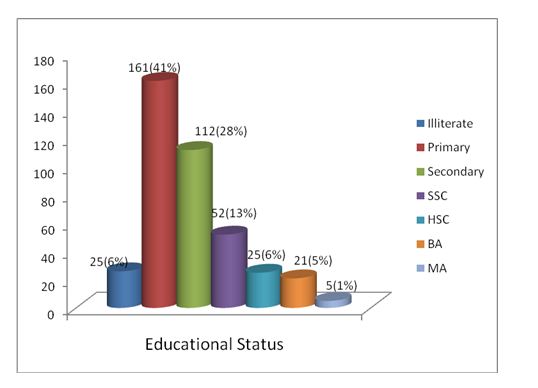 The above table shows the educational status of the study population. Among the total 402 respondents, majority 141 (41%) had primary level of education, followed by 98 (28%) had secondary level. Only 6% were illiterate.
The above table shows the educational status of the study population. Among the total 402 respondents, majority 141 (41%) had primary level of education, followed by 98 (28%) had secondary level. Only 6% were illiterate.
Distribution of respondents by sex and area of residence
Area of residence | Sex | Total | |
Male | Female | ||
| Urban | 70 | 132 | 202 |
35% | 65.% | 100.0% | |
| Rural | 99 | 101 | 200 |
49% | 51% | 100.0% | |
| Total | 169 | 233 | 402 |
42.0% | 58.0% | 100.0% | |
The above table shows that among the respondents, in urban area 35% (n=70) were male were and 65% (n=132) were female and among the rural respondents 49% (n=99) were male and rest 51% (n=l0l) were female.
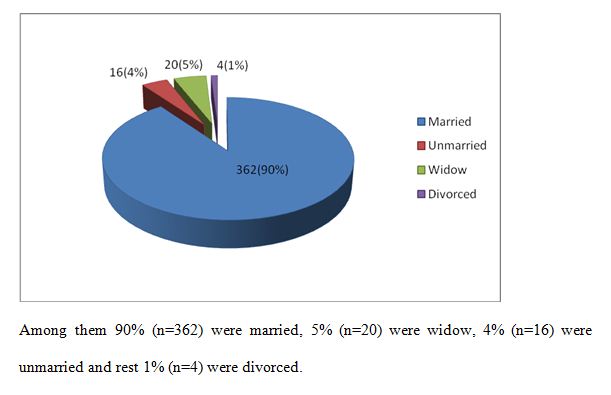
Distribution of respondents by marital status
DISCUSSION
In this study, from urban area one third male and two third female and from the rural respondents about same ratio of male and female were included as participants. Among them ninety percent were married, five percent were widow, four percent were unmarried. By religion almost ninety six percent were Muslim; near about four percent were Hindu. By occupation half of respondents were housewives, followed by less than one fifth were service holder, one-tenth were business person and rests were engaged in agricultural work and daily labor. By educational status of the study population, forty percent had primary level of education, followed by less than one-third had secondary level of education. By monthly family income, one-third had monthly income up to 10000 tk, less than one-third had 10001 to 20000 tk,
Among the respondents of the study two-third answered the correct BP reading for hypertension. By symptoms of hypertension, Headache (91.5%), Neck-pain (74.9%), Vertigo (63.4%) was reported by the respondents during the study. As risk factors of hypertension, mental Stress (93.3%), Age (58.6%), fat (52.1%), Positive family history (49.9%) Smoking (42.4%), Obesity (31.7%) and Diabetes (30.7%) were mentioned by the respondents. Study by Kishimoto et al25 among rural and urban Vietnamese and Japanese outpatients found that excessive sweet intake, lack of exercise, and obesity were cited as risk factors for diabetes by the urban Vietnamese and Japanese subjects. The most commonly cited risk factor for hypertension by the Japanese subjects was excessive salt intake, whereas obesity and alcohol consumption were cited by the urban and rural Vietnamese subjects, respectively. In both countries, medical information was mainly obtained from medical staff, but other mass media were also commonly used as sources of information. Among the 155 rural Vietnamese subjects, 18(11.6%) were hypertensive, and 7 (38.9%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. The rural Vietnamese subjects considered excessive alcohol consumption (87.1%), obesity (83.9%), and smoking (80.6%) as the 3 major risk factors for hypertension, and 70.3% of these people identified excessive salt intake, which ranked seventh among the 9 factors listed in the questionnaires, as a risk for hypertension. Among the 147 urban Vietnamese subjects, 33 (22.4%) were hypertensive, and 11 (33.3%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. The urban Vietnamese subjects considered obesity (79.6%), aging (78.9%), and excessive alcohol consumption (77.6%) to be the 3 major risk factors for hypertension. Although 66.7% of the urban Vietnamese subjects identified excessive salt intake as a risk factor for hypertension, it was ranked eighth among the 9 factors listed in the questionnaires (Figure 2b). Among the 102 urban Japanese subjects, 13 (12.7%) were hypertensive, and 10 (76.9%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. In all, 80.4% of the urban Japanese subjects considered excessive salt intake as a risk factor for hypertension, which was the most frequently selected choice among the listed risk factors. Among the 159 Japanese outpatients, 58 subjects (36.5%) were hypertensive, and 49 (84.5%) of these hypertensive subjects stated that they were aware of the risk factors for hypertension. In all, 69.8% of the Japanese outpatients considered excessive salt intake as a risk factor for hypertension; it was the most frequently selected option among the listed risk factors. The patterns of the results for all the patients and for the hypertensive patients were quite similar.
As complications of hypertension three fourth mentioned Heart attack, forty percent mentioned Heart failure, about half mentioned Eye problem (Blindness), about eighty percent told Stroke and one fourth mentioned Kidney failure.
To control hypertension almost ninety percent mentioned ) intake of low fat, three-fourth mentioned intake of low salt, more than sixty percent intake of more vegetable, forty percent mentioned intake of more Fruits and less than half mentioned not to consume any alcohol.
As preventive measure for hypertension all of the respondents mentioned that monitoring of blood pressure is most effective preventive measure while half of the respondents mentioned frequent Electrocardiogram (ECG) is necessary for prevention of hypertension.
As management for hypertension more than ninety percent of the respondents mentioned regular intake of Drug/Medication followed by three-fourth Diet control, less than half Regular exercise (Walking at least 30 minutes a day) and forty percent mentioned Diet control and exercise. Study in Kerala (South India) found that only 81 (16.8%) hypertensive patients were aware of their disease. Among the parameters such as dietary habits, physical activity, educational standards, salt intake, and diabetes mellitus, only high salt diet (P= 0.03) and diabetes mellitus (P= 0.004) had a significant association with hypertensive state20. In Canadian study majority were unaware of the association between hypertension and heart disease (80%), heart attack (66%), kidney disease (98%), damage to blood vessels (95%) and premature death (74%). Respondents also had limited knowledge of lifestyle issues affecting hypertension, despite 44% indicating that they were overweight and 18% identifying themselves as smokers. Almost two-thirds (63%) thought hypertension had clearly identifiable signs or symptoms, although they believed that hypertension was not a serious medical condition. Most respondents (59%) falsely believed that they would not develop hypertension and 38% thought that they would be able to control hypertension without the aid of a physician if they did have hypertension22.
For prevention of hypertension, almost all of the respondents mentioned avoid smoking, taking fruits and vegetable rich but low-fat diet, avoiding alcohol consumption are the ways of prevention hypertension.
The study revealed that most of the respondents (82.4%) reported that when one person feel any physical problem/ sickness should consult with doctor, but half mentioned that when blood pressure goes beyond normal then one should call doctor.
By knowledge level, it was found that among the respondents about sixty percent had poor knowledge, less than thirty percent had moderate knowledge and rests had satisfactory level of knowledge. Among the respondents, poor knowledge was found more among urban people than rural people, moderate level of knowledge was found among urban population than rural population and satisfactory level of education was found more among urban population than rural (p>0.05). Poor knowledge was observed among female than male, moderate level of knowledge was observed more among male than female and satisfactory level of knowledge was observed more among male than female (p>0.05). Study in USA reported that the awareness was low among the young, but increased with older age. The popular belief that hypertension and diabetes mellitus are diseases of the elderly may be the reason for the low level of awareness among the youth. Improving awareness in the community is an important population-based strategy for prevention of complications of these diseases12.
CONCLUSION
The study concluded that among the respondents about sixty percent had poor knowledge, less than thirty percent had moderate knowledge and rests had satisfactory level of knowledge regarding risk factors and complication of hypertension. Poor knowledge was found more among urban people than rural people and female compare to male. The knowledge gap among urban people compare to rural people could not be identified. This finding demands further study on large sample to find out the possible explanation.
RECOMMENDATION
- To improve knowledge regarding risk factors and complication of hypertension, awareness program should be conducted properly to the urban and rural population.
- Identification of the target group for hypertension and community health education campaign regarding hypertension should be strengthening.
- For developing knowledge and awareness for hypertension mass media should be used with key message and should be accessible to community people.